UNIT 3 What Is Most Concerning?
INTRODUCTION
Chapter 1 – Gross & Fine Motor Skills
PART 1 – Poor Eating
PART 2 – Toilet Training
Chapter 2 – Speech & Language Communication (Including 'Nonverbal' &
assisted/alternative)
Chapter 3 – Cognition, Theory of Mind, & Temperament/Personality
Unit 3 – REFERENCES
Unit 3 – APPENDIX A Learning Disabilities APPENDIX B Theory of Mind (ToM)
PLEASE READ DISCLAIMER –
UNIT 3 WHAT IS MOST CONCERNING?
CHAPTER 2 – SPEECH & LANGUAGE COMMUNICATION (Including non-verbal & assisted alternative speech)
INTRODUCTION
Chapter 1 – Gross & Fine Motor Skills
PART 1 – Poor Eating
PART 2 – Toilet Training
Chapter 2 – Speech & Language Communication (Including 'Nonverbal' &
assisted/alternative)
Chapter 3 – Cognition, Theory of Mind, & Temperament/Personality
Unit 3 – REFERENCES
Unit 3 – APPENDIX A Learning Disabilities APPENDIX B Theory of Mind (ToM)
PLEASE READ DISCLAIMER –
UNIT 3 WHAT IS MOST CONCERNING?
CHAPTER 2 – SPEECH & LANGUAGE COMMUNICATION (Including non-verbal & assisted alternative speech)

INTRODUCTION –
Bradshaw & Klainman (2018) are persuaded that Autism Spectrum Disorder (ASD) is characterized by impairments in motor activity, social interaction, and deficits in communication. They believe the ‘communication predictor’ is determined by how well a child is able to appropriately use both ‘expressive’ and ‘receptive’ language, early in life.
As addressed in the study, ‘expressive’ speaking is using language appropriately. It is having the ability to express wants, needs, ideas, and thoughts in a meaningful way; while using words to engage in ‘back-and-forth’ conversation.
‘Receptive’ listening is understanding spoken language. It is having the ability to gain meaningful information from words which are communicated in commands, questions, and phrases which are directed specifically to them. Again, understanding what is being said, in order to engage in ‘back-and-forth’ conversation.
Other ASD predictors they mention are connected to ‘independent walking’ by the age of 1 year old. Early ‘independent walking’ opportunities affords the child with new experiences and new visual perspectives. ‘Walking’ is also important to predicting a child’s normal development and how efficiently he or she takes on locomotion between objects of interest, and/or in a way to reach out to caregivers. It is an important predictor of normal development because ‘purposeful locomotion’ increasingly motivates the child to actively explore his or her world.
Kover, et al. (2016) talk about a study which examines the child’s early ‘speech’; saying their first words and first phrases are predictive of the developmental trajectories of functional behavior.
In early childhood, it is expected that a child should produce at least 10 words, by the age of 18 months. And, that the child’s ‘first words’ should consist of ‘useful speech and language’. It is important that by the age of 5 years old, the child is appropriately using useful ‘expressive’ language, and that they are able to understand purposeful ‘receptive’ language.
What is communication? Stokes (2018) says – ‘Communication’ is a range of purposeful behavior which is used with intent within the structure of social exchanges, to transmit information, observations, or internal states; or to bring about changes in the immediate environment. Nonverbal behaviors are included, as long as some intent, evidenced by anticipation of outcome can be inferred.
Speech/verbalization becomes communication when there is a desire or intent, to convey a message to someone else. A child’s ‘expressive’ language level does not necessarily speak to his or her cognitive level.
In some disorders (e.g., autism) cognitive ability may be higher than one’s observable language skills, especially ‘expressive’ language skills. When developing learning activities, teachers and parents must figure out which types of activities are appropriate for both the child’s mental and chronological ages. Plus, a big success factor can be found when addressing the individual’s area of interest.
Because social relations are a primary area of difficulty for children with autism, it is not surprising that effective social communication is significantly impaired for these children. Both the areas of communication and social skills are tightly interwoven and interdependent.
Therefore, the development of communication skills cannot be the sole responsibility of the speech/language pathologist. While s/he may provide the ‘guide posts’ and strategies, communication must be continually addressed by everyone coming in contact with the child.
< My Thoughts > “…communication must be continually addressed …”
When the newborn baby cries out its probably to satisfy a ‘sensory’ need – I’m hungry, I’m hot/cold, I’m wet, I’m uncomfortable! These desperate cries are primal sounds made in hopes of getting a comforting response from whomever is within earshot.
When answering these cries, whether from a newborn or a toddler, try to keep to an approach which will help your child feel cherished and worthy of all the fuss. If a child’s needs are not easily met, in the only way in which s/he is capable of communicating, then it’s possible that the ‘primal screaming’ infant will reemerge.
Remember, s/he is not trying to ‘give’ you a bad time – s/he is ‘having’ a bad time!
Know too, that throughout childhood, kiddos hear and understand ‘receptive’ language much, much more than we think that they do. From the very beginning, they also ‘pick up’ on your attitude and feelings. Studies show that sensitive children see how people really feel through the ‘auras’ which surround that person.
Your neurotypical child may say, “The teacher doesn’t like me.” What the autistic child can’t always express is that they feel unwanted because when their teacher approaches, her aura turns brown. Brown is a ‘yucky’ color, like dirt and other unpleasant things.
Whippery (2019) wants us to know that autistic children and adults when under stress may see ‘auras’ around people or sounds. This is known by scientists as ‘synesthesia’, which is caused by hyper-excitability of the visual cortex. But even loud or unusual sounds can trigger this kind of event. The person dealing with a child experiencing a synesthesia event, may find that the child suddenly becomes uncooperative or overly excited.
SPEECH (Including – ‘non-verbal, alternative/assisted)
Mukhopadhyay (2011) – I could see the green curtains move with the breeze. I could see the leaves of the Sal-trees move, and I could see the ceiling fan move.
Even my hands moved when I flapped them. Only my lips would not move.
My thoughtful mind would wonder about the sound of my talking voice, which I could only hear when I laughed or screamed.
I promised the mirror that I would remember not to distract it with all my talking, especially when it showed me stories of the wind, and the ceiling fan, or the color of air. I promised the mirror with complete sincerity. The mirror reflected back my promise with total earnestness.
< My Thoughts > “…stories of the wind…”
Some years later, Tito’s mother helped him put his ‘stories’ on paper for all to read. Through his need to communicate his stories, her development of Facilitated Communication became available to the world.
Note: More about Facilitated Communication (FC) in Unit 7 CAMs, Part 4-8; and PECS, Unit 7, Ch. 2, Sec. 2.
Driver (2011) determines that developing communication skills will be difficult for those affected with autism. But there are many strategies you can employ, because we are born to communicate. Improve communication with a child and you will reduce frustration, tantrums and emotional outbursts.
< My Thoughts > “…Improve communication with a child.”
Some parents know what their child wants because s/he drags them there, or, they scream until you figure it out. It’s sort of like the old game of ‘Charades’. Okay, you’re getting warmer, almost there! Nope! Wrong way, getting cold! You may see a look of confusion when you ask your child what s/he wants because they think you know what they want, but you just don’t want them to have it.
Sonny is ‘non-verbal’, or as some say ‘non-vocal’. He doesn’t say any words so he’s non-verbal, but he really isn’t ‘non-vocal’ because when you say, “Show me what you want,” he may vocalize a noise. That noise can be a grunt to mean “Okay, I’ll show you, but with my eyes or touch.” And then when you say, “Sonny, is this what you want?”, he may smile (That’s it!). Or, he may ‘grunt’ (Nope! Try again!”); as he is continuing to try to guide you towards what he wants.
Sometimes Sonny’s response or sign is so subtle that you can miss it all together. Or, just when you think that you’ve got it and have all the clues, he presents you with a whole set of new responses! Then, he may revert back to signs or responses we haven’t seen in years; maybe just to see if we’re really paying attention. And, so it goes.
Stokes (2018) says that what a young child is able to express to you is so limited, because for them to get the thoughts in their mind to come out of their mouth is an extremely complex, highly developed cognitive function. So, give your child a way to get your attention and send you into action, other than with a tantrum. And, don’t forget to teach family members and caregivers how to interpret the ways that your child is using to communicate their wants and needs, especially if it’s through sign language or communication devices.
< My Thoughts > “…communicate their wants and needs…”
Having a non-verbal autistic child, as Sonny is, puts an extra strain on our communication. Early on, we learned to ask him, “Show me what you want.” Of course, this exacerbated his tendency to drag us to what he wanted, or to where he wanted us to go. Eventually, before we all became too frustrated, we taught him and he began using ‘baby signing’. Then, he learned to use his low technology ‘Cheap Talk’ communication device to summon us. We also have a similar small push-button device which we take with us in the car.
Bradshaw & Klainman (2018) are persuaded that Autism Spectrum Disorder (ASD) is characterized by impairments in motor activity, social interaction, and deficits in communication. They believe the ‘communication predictor’ is determined by how well a child is able to appropriately use both ‘expressive’ and ‘receptive’ language, early in life.
As addressed in the study, ‘expressive’ speaking is using language appropriately. It is having the ability to express wants, needs, ideas, and thoughts in a meaningful way; while using words to engage in ‘back-and-forth’ conversation.
‘Receptive’ listening is understanding spoken language. It is having the ability to gain meaningful information from words which are communicated in commands, questions, and phrases which are directed specifically to them. Again, understanding what is being said, in order to engage in ‘back-and-forth’ conversation.
Other ASD predictors they mention are connected to ‘independent walking’ by the age of 1 year old. Early ‘independent walking’ opportunities affords the child with new experiences and new visual perspectives. ‘Walking’ is also important to predicting a child’s normal development and how efficiently he or she takes on locomotion between objects of interest, and/or in a way to reach out to caregivers. It is an important predictor of normal development because ‘purposeful locomotion’ increasingly motivates the child to actively explore his or her world.
Kover, et al. (2016) talk about a study which examines the child’s early ‘speech’; saying their first words and first phrases are predictive of the developmental trajectories of functional behavior.
In early childhood, it is expected that a child should produce at least 10 words, by the age of 18 months. And, that the child’s ‘first words’ should consist of ‘useful speech and language’. It is important that by the age of 5 years old, the child is appropriately using useful ‘expressive’ language, and that they are able to understand purposeful ‘receptive’ language.
What is communication? Stokes (2018) says – ‘Communication’ is a range of purposeful behavior which is used with intent within the structure of social exchanges, to transmit information, observations, or internal states; or to bring about changes in the immediate environment. Nonverbal behaviors are included, as long as some intent, evidenced by anticipation of outcome can be inferred.
Speech/verbalization becomes communication when there is a desire or intent, to convey a message to someone else. A child’s ‘expressive’ language level does not necessarily speak to his or her cognitive level.
In some disorders (e.g., autism) cognitive ability may be higher than one’s observable language skills, especially ‘expressive’ language skills. When developing learning activities, teachers and parents must figure out which types of activities are appropriate for both the child’s mental and chronological ages. Plus, a big success factor can be found when addressing the individual’s area of interest.
Because social relations are a primary area of difficulty for children with autism, it is not surprising that effective social communication is significantly impaired for these children. Both the areas of communication and social skills are tightly interwoven and interdependent.
Therefore, the development of communication skills cannot be the sole responsibility of the speech/language pathologist. While s/he may provide the ‘guide posts’ and strategies, communication must be continually addressed by everyone coming in contact with the child.
< My Thoughts > “…communication must be continually addressed …”
When the newborn baby cries out its probably to satisfy a ‘sensory’ need – I’m hungry, I’m hot/cold, I’m wet, I’m uncomfortable! These desperate cries are primal sounds made in hopes of getting a comforting response from whomever is within earshot.
When answering these cries, whether from a newborn or a toddler, try to keep to an approach which will help your child feel cherished and worthy of all the fuss. If a child’s needs are not easily met, in the only way in which s/he is capable of communicating, then it’s possible that the ‘primal screaming’ infant will reemerge.
Remember, s/he is not trying to ‘give’ you a bad time – s/he is ‘having’ a bad time!
Know too, that throughout childhood, kiddos hear and understand ‘receptive’ language much, much more than we think that they do. From the very beginning, they also ‘pick up’ on your attitude and feelings. Studies show that sensitive children see how people really feel through the ‘auras’ which surround that person.
Your neurotypical child may say, “The teacher doesn’t like me.” What the autistic child can’t always express is that they feel unwanted because when their teacher approaches, her aura turns brown. Brown is a ‘yucky’ color, like dirt and other unpleasant things.
Whippery (2019) wants us to know that autistic children and adults when under stress may see ‘auras’ around people or sounds. This is known by scientists as ‘synesthesia’, which is caused by hyper-excitability of the visual cortex. But even loud or unusual sounds can trigger this kind of event. The person dealing with a child experiencing a synesthesia event, may find that the child suddenly becomes uncooperative or overly excited.
SPEECH (Including – ‘non-verbal, alternative/assisted)
Mukhopadhyay (2011) – I could see the green curtains move with the breeze. I could see the leaves of the Sal-trees move, and I could see the ceiling fan move.
Even my hands moved when I flapped them. Only my lips would not move.
My thoughtful mind would wonder about the sound of my talking voice, which I could only hear when I laughed or screamed.
I promised the mirror that I would remember not to distract it with all my talking, especially when it showed me stories of the wind, and the ceiling fan, or the color of air. I promised the mirror with complete sincerity. The mirror reflected back my promise with total earnestness.
< My Thoughts > “…stories of the wind…”
Some years later, Tito’s mother helped him put his ‘stories’ on paper for all to read. Through his need to communicate his stories, her development of Facilitated Communication became available to the world.
Note: More about Facilitated Communication (FC) in Unit 7 CAMs, Part 4-8; and PECS, Unit 7, Ch. 2, Sec. 2.
Driver (2011) determines that developing communication skills will be difficult for those affected with autism. But there are many strategies you can employ, because we are born to communicate. Improve communication with a child and you will reduce frustration, tantrums and emotional outbursts.
< My Thoughts > “…Improve communication with a child.”
Some parents know what their child wants because s/he drags them there, or, they scream until you figure it out. It’s sort of like the old game of ‘Charades’. Okay, you’re getting warmer, almost there! Nope! Wrong way, getting cold! You may see a look of confusion when you ask your child what s/he wants because they think you know what they want, but you just don’t want them to have it.
Sonny is ‘non-verbal’, or as some say ‘non-vocal’. He doesn’t say any words so he’s non-verbal, but he really isn’t ‘non-vocal’ because when you say, “Show me what you want,” he may vocalize a noise. That noise can be a grunt to mean “Okay, I’ll show you, but with my eyes or touch.” And then when you say, “Sonny, is this what you want?”, he may smile (That’s it!). Or, he may ‘grunt’ (Nope! Try again!”); as he is continuing to try to guide you towards what he wants.
Sometimes Sonny’s response or sign is so subtle that you can miss it all together. Or, just when you think that you’ve got it and have all the clues, he presents you with a whole set of new responses! Then, he may revert back to signs or responses we haven’t seen in years; maybe just to see if we’re really paying attention. And, so it goes.
Stokes (2018) says that what a young child is able to express to you is so limited, because for them to get the thoughts in their mind to come out of their mouth is an extremely complex, highly developed cognitive function. So, give your child a way to get your attention and send you into action, other than with a tantrum. And, don’t forget to teach family members and caregivers how to interpret the ways that your child is using to communicate their wants and needs, especially if it’s through sign language or communication devices.
< My Thoughts > “…communicate their wants and needs…”
Having a non-verbal autistic child, as Sonny is, puts an extra strain on our communication. Early on, we learned to ask him, “Show me what you want.” Of course, this exacerbated his tendency to drag us to what he wanted, or to where he wanted us to go. Eventually, before we all became too frustrated, we taught him and he began using ‘baby signing’. Then, he learned to use his low technology ‘Cheap Talk’ communication device to summon us. We also have a similar small push-button device which we take with us in the car.

Hoecker (2018) has information that limited research suggests that ‘baby sign language’ might give a child a way to ease communication frustrations between 8 months and 2 years. During those years, children begin to know what they want but don’t always have the verbal skills to express themselves. There are many ideas when you are searching on your own for sources about teaching ‘baby sign language’.
< My Thoughts > “…ease communication…”
While you are waiting for diagnosis or doctors and professionals to help you, you can start with what is called ‘baby signing’. Depending on the level of your child’s ability to communicate, there are also adaptable ‘low tech’ devices.
Baby signing usually works because many children with autism are very visual, and will respond to early or ‘baby’ signing. Signs for – eat, drink, stop, wait, bed, toilet, stand-up, sit-down, help, finished, etc. Just so you know, very small neurotypical infants can learn how to sign.
Most babies learn to wave ‘bye-bye’, throw a kiss, and nod their head for ‘yes’ or ‘no’. Sonny will blink his eyes for ‘yes’ and ‘no’, but never nods. Don’t know why, but children with autism often make-up their own gestures. Even if they make-up signs, as Sonny does, it’s still ‘communication’ as long as you both know what it means.
Hoecker has ways that you may learn ‘baby signing’, on YouTube videos, in eBooks, to give you a start. Trying them, may surprise you. But he cautions that the first sign language attempts by your child will look like loose gestures, not the real signs.
Be patient and pay attention, because they will be upset if you don’t pick up their sign interpretation right away.
< My Thoughts > “Be patient and pay attention…”
When children make up their own signs it’s up to you to figure out the sign’s meaning, before the storm builds and the tantrum comes. Sonny slaps his thighs which can mean something’s funny, or that he’s getting anxious about something; or that he’s trying to ‘sign’ something. In either case, he wants us to join in. He is participating in your world and expects you to respond to this ‘thigh slapping’ communication. Also, he may hit his head with an open hand or his knuckles. This can mean that he’s experiencing anxiety, seizure activity or that he just thought of something really funny, but it’s also a communication of sorts.
He often improvises, for instance, the sign for ‘more’ is to gesture with both hands, putting fingertips together several times. Sonny’s interpretation at first was to clap his hands together, because clapping was what he already knew how to do. And eventually, he was able to better approximate the sign for ‘more’, but he still claps his hands first, or slaps his thigh to alert us that he is signing something.
Hoecker says help your child communicate wants and needs to prevent tantrums. And, that it’s up to you to teach all family members and caregivers how to interpret the signing that your child is doing to communicate wants and needs. Maybe there is some sort of ‘alert’ before the sign is coming.
< My Thoughts > “…‘alert’ before the sign is coming.”
Sonny also claps his hands loudly if he can’t remember a sign, or if I’m ‘not getting the sign, he will improvise something. If he forgets the sign for ‘hurry’ he will frantically give the sign for ‘more’ – as in ‘more faster’ I guess.
Another method of communication for Sonny are his interactive children’s books. Some of his favorites are – Sesame Street Elmo’s Play-a-Sound Pop-Up Song Book, Mickey Mouse Play-a-Song with Piano Keys, Nickelodeon Dora and Diego Interactive Sound Books. All of these are board books and take a lot of use and abuse, but have phrases he likes.
One of the reasons they’re his favorites are because he also uses them for communication, especially on certain occasions. It’s one of the Dora books which has a button that when pushed says, “Vamonos!, Let’s go!” He usually takes this when we have an appointment. He pushes it repeatedly to let everyone in the office know he is tired of waiting for the doctor or whomever.
Then there’s the Mickey Mouse book which has a button that when pushed says – “Oh Boy! Come on! Let’s GO!” He has this in the kitchen, to use when I’m not filling his cup fast enough. Then he laughs. Yes, he has quite a sense of humor, autism and all. Sonny’s MA (mental age) is between that of a 2 of 3-year-old. So, if he can do this kind of improvisation, your child should be a whiz!
Stagliano (2010) says that the photographs of her daughter as a toddler show a beaming girl, happy to flirt with the camera. She made eye contact and also used imaginative play. But she cautions that her Mia never called out to her. She cried and came to get me when she needed something, but she never used her voice to attract my attention. A warning sign I missed.
< My Thoughts > “…Never used her voice…”
There is anecdotal evidence of this in parent interviews, that more often than not, a nonverbal child will seek out the nearest someone, grab them by their most easily reachable body part and attempt to drag them to whatever is wanted or needed. Reports of this covert maneuver seems to be absent in the professional literature.
With Sonny we found ourselves saying, “Show me what you want,” which resulted in him, as he begun dragging us to the refrigerator, or the toy room. So, which came first, our asking him to show us what he wanted; or, his instinctively dragging us to what he wanted? Honestly, I don’t know. This is where use of even the most elementary ‘baby’ sign language can eliminate a lot of frustration and tears, for both child and parents.
But, Driver (2011) discusses that developing language and communication skills may be difficult for those affected with ASD. And, how understanding the way your child is expressing ‘wants’ and ‘needs’ will take patience and understanding on everyone’s part.
< My Thoughts > “…expressing ‘wants’ and ‘needs’
Most likely at some point, your child will have a speech therapist help them with the communication to express their ‘wants’ and ‘needs’. Developing communication goals frequently becomes one of the first interventions to be recommended.
WebMD Contributor (2020) considers that a speech therapist delivering an individualized treatment is crucial. An experienced speech therapist, working closely with a team of child psychologists and others can provide the communication and behavior supports the child needs. This would be the most desirable situation for everyone.
Speech therapy techniques may include –
- Using electronic ‘talkers’
- Signing or typing devices
- Pointing to picture boards
- Implementing picture exchange communication systems (PECS)
- Gaining tolerance for sounds with which person has sensory issues
- Improving articulation by massage or therapy techniques
- Singing songs with individuals to improve speech and reduce stress
< My Thoughts > “…techniques may include…”
These are just some of the techniques of a Speech-Language Pathologist (SLP). All children seem to learn best when they are having fun or gaining something pleasurable from the experience.
Stress and frustration can be our enemies. Often behavior improves a thousand percent when the child has effective ways of communicating, albeit with visual cue cards, augmented communication devices, signing, or typing on the computer.
Early speech therapy intervention to assist the individual’s grasp of spoken language and the need for communication should start as soon as a language delay is suspected. Usually between 10 – 18 months of age, according to this WebMD contributor.
Squaresky (2014) says at age two, when son Greg’s speech regressed, we worried about his hearing. He still sang entire songs and recited the alphabet with Sesame Street’s Bert and Ernie, yet he had no conversational ability whatsoever. Speech therapy brought little change as the most I heard Greg mutter during each session was one word. Generally, he repeated what Laura said, a phenomenon known as echolalia (parroting speech). I wanted conversation. Two words, three words, a sentence, maybe?
Piven (2015) puts ‘echolalia’ in the category of a repetitive and stereotypical characteristic of autism.
Whiffen (2009) wants us to know, that almost two years since Clay’s diagnosis, his speech and language skills now are testing consistently within normal limits, on assessments. Vocal tone, pitch, prosody, and rhythm are adequate. Clay’s learning and memory skills were also within normal limits. He demonstrated an age-appropriate ability to shift and direct attention, and to filter extraneous stimuli to acquire information.
< My Thoughts > “…testing consistently within normal limits.”
During these two years with Clay, Leeann has had him in a variety of programs, consecutively. So, it’s really difficult for an outsider to separate out the results of just one of the programs. As many parents find, because of the need to work on behavior challenges, programs may coincide.
Another factor may be that the expensive programs for which a child may qualify, or may receive, will also be provided ‘free’ as a ‘school’ or ‘community’ service. Focusing on the progress is the main thing, and the hope that with the appropriate intervention, things may change.
As the doctor continues speaking, I begin to feel as light as a seed pod blowing through the air. Each time she says ‘average’ or ‘above average’, I want to jump up and do the victory dance.
LANGUAGE COMMUNICATION (Including nonVerbal, assisted/alternative)
Autism Consultant Stokes (2018) believes that “the child must be able to understand the ‘purpose’ of the communication.” Does the child have or understand the “need” to communicate? What is the payoff for the child? How and what is your child communicating and how will you know? Developing some type of communication is an essential first step.
Having some form of early communication is extremely important because it helps with the following:
- Reduces frustration
- Lessens emotional outbursts
- Increases parent/child bonding
- Establishes self-esteem
- Starts to promote feelings of satisfaction and control
So, it’s huge to be able to know what they want and what they don’t want. Later, you can move on to a more sophisticated communication program. Understand that the ‘BEHAVIOR’, tantrum or meltdown you are seeing in your child is sometimes their ONLY form of COMMUNICATION.
< My Thoughts > “…tantrum or meltdown…”
The difference between knowing when your child is throwing a tantrum and when s/he is having a sensory meltdown is important to know.

Mayo Clinic Staff Writer (2018) explains that temper tantrums frequently occur because young children are not equipped to express frustration in other ways. Even their limited vocabularies can make them feel frustrated to the point of tantrumming. That’s an anatomy of tantrums.
Perhaps the child wants a toy but doesn't have the power to convince the parent... (as the child who is being denied something he wants).
Perhaps the child wants a toy but doesn't have the power to convince the parent... (as the child who is being denied something he wants).

Or, perhaps s/he wants to stay somewhere, but the parent says that it's time to go. These events can turn into tantrums, especially when children are put in situations that can spark strong emotions and there is an interested audience. The behavior typically subsides once the child gets enough attention or, has his or her wants met.
For a ‘tantrum’ the child needs an audience. Tantrums are angry or frustrated outbursts. They are a purposeful performance, expecting a rewarding reaction from their onlookers. These are children looking for a certain response to their performance.
For a ‘tantrum’ the child needs an audience. Tantrums are angry or frustrated outbursts. They are a purposeful performance, expecting a rewarding reaction from their onlookers. These are children looking for a certain response to their performance.

Brain Balance Contributor (2014) explains that a ‘sensory meltdown’ is an incident which occurs when unwanted sensory input floods the child’s brain. Once that happens, some experts think the child’s ‘fight or flight’ response takes over. This excess input ‘overflows’ in the form of yelling, crying, lashing out, or running away. To manage a meltdown, help the child find a safe, quiet place to de-escalate. “Let’s leave the store and sit in the car for a few minutes.” Then provide a calm, reassuring presence without talking too much to your child. Maybe play his or her favorite music. The goal is to reduce the agonizing input coming at them and replacing it with something soothing to them.
Knowing the difference between tantrums and meltdowns is the key to helping a child through them. It may also help to get a better idea of the kinds of situations that can be challenging for your child. You can also explore tips on how to deal with noise and other sensitivities.
< My Thoughts > “…challenging for your child.”
Challenging for you too, because the difference between a sensory meltdown and a temper tantrum may not be easy to determine, the first time or two. The problem with trying to unlock a child’s sensory needs is that what may be frightening or even terrifyingly unbearable one time may become stimulating and sensory-seeking to the child or student the next time.
Aggression, violence, and other challenging behavior may really be signs of Sensory Issues. Denman, et al. (2016) say – Families of a child diagnosed with autism can find themselves trying to understand their child’s behavior while on the waiting list for ‘formal diagnosis.’ How this ‘parental making sense’ of behaviors affects parenting in the meantime is important. Confusions can also occur for the children who have insecure attachment patterns as well as sensory impairments.
For instance, parents may have difficulty understanding how a slight change in routine can cause a child to have a sensory ‘meltdown’, in the middle of the street. At the same time, parents may be more concerned about the need to present a ‘positive parenting identity’ to friends, family members, or others who are viewing the ‘middle of the street meltdown’.
< My Thoughts > “…viewing the ‘middle of the street meltdown’.…”
When viewing that ‘middle of the street meltdown’, an uninformed society may be determined they are seeing a ‘bad kid’ or ‘bad parenting’, or both. But, AGAIN, “He’s not giving you a bad time.” “He’s having a bad time.”
Note: More about ‘sensory’ behavior in SENSORY UNIT 4
Barnes (2014) relates this – Our son, who we call the Navigator, and I stopped for lunch at a fast-food restaurant. We made it in okay, and finally to the front of the line. It was lunchtime, crowded, with lots of noisy activity. Navigator, began being unable to process the noisy sensory input. He looked up at me. “Do you need to go outside?” He nodded; his eyes large. We went outside and placed our order there. While we waited, my son explored in detail the mysteries of the asphalt parking lot.
Duan-Young (2014) explains that the sound Aimee let out was like something you’d imagine a wild animal would make. First the bed clothes were ripped off the bed. Next, the mattress came off the bed. Aimee had recently come to live in our group home and this was her way of ‘communicating’.
Aimee was not able to verbally communicate. When she became frustrated, or wanted something and didn’t know how to express herself, she would do the only thing she knew. She would become physically violent and destroy whatever was near her.
From a behavioral analyst’s point of view, every behavior has a function, or intent. One of the ‘mistakes’ parents make when children calm down after a tantrum is ask them “Why did you do that?” “Didn’t I tell you that you’re not supposed to do that?” “What’s wrong with you?”
Greene (2014) gives us a newer approach to understanding and parenting the child who seems to be easily frustrated and frequently inflexible. Here are some of Dr. Greene’s Plan B Steps, when Plan A isn’t working – Step 1 is the Empathy Step and is followed by Step 2, the Identify the Problem Step; and Step 3 is the Invitation Step.
< My Thoughts > “…Dr. Greene’s Plan B Steps…”
My version of adapting Plan B steps would go something like this for a neuro-typical child. But needing more adaptation for a child with autism, yet keeping the ‘empathy’ theme.
Step 1 is the Empathy Step
Parent: I’ve noticed that you’ve been struggling a lot over doing your chores lately. What’s up?
Step 2 is the Identify the Problem Step
Child: It’s too hard.
Parent: Which part’s too hard?
Child: There’s too much.
Step 3 is the Invitation Step
Parent: How about taking some time and writing down the chores you don’t mind doing and the ones you don’t want to do. Maybe we can shorten the list, or change some of your choices.
Dr. Greene asks us to keep in mind that every child is at different stages in their emotional and social development. Sometimes the very bright and more astute children have the most difficulty in life, because they ‘know’ that there are many ‘injustices’ or ‘perceived injustices’ in their world. And, they are considerably unhappy until ‘justice’ is served, so to speak.
< My Thoughts > “…‘perceived injustices’…”
This is especially true of the ‘literal thinking’ autistic children and adults. Beware, ‘perceived injustices’ may be cause for a sudden tremendous tantrum.
Shalom, et al. (2006) states that the participants with autism who could express themselves about feelings stated the following – Mostly they only had ‘conscious’ feelings about things which were ‘pleasant’ versus ‘unpleasant’ or, ‘interesting’ versus ‘boring’
Decker (2013) says sometimes her autistic son Jaxson resembles the devil incarnate. But when he smiles, he lights up a room.
“Stars!” “Stars!” Jaxson insists.
“Stars?” I answer back.
“Stars, yes,”
“Stars?” We went back and forth like that for two minutes. He wanted something from me and if I couldn’t figure out what he wanted, in the next twenty seconds or so, ‘you know what’ would be hitting the fan – or the walls. Biting hitting, screaming, kicking – any or all of the above were imminent.
He was doing his part – he was asking. I just wasn’t equal to the task. I had no idea what ‘stars’ meant in his strange little world.
“Stars!” I could see the urgency bubbling up within him. He tilted his head, thinking a minute, the synapses firing in his special brain. “DS?” he inquired.
“DS? You want your Nintendo DS?” He wanted his game! “DS, please.” What stars had to do with DS I had no idea. But you have to love an autistic kid who can still use the word ‘please’.
< My Thoughts > “Nintendo DS…”
On the Nintendo website they tell us that ‘star coins’ can be earned at all levels of the Nintendo DS game. Could it have been earning ‘star coins’ that Jaxson connected with, as a way to communicate that he wanted to play his Nintendo DS?
And, what was the game’s attraction for Jaxson? Probably, as for many players, the chance to interact with the world through action games without leaving the security of his room. For the autistic child, if it improves eye-hand coordination, and possibly even gives him better spatial orientation, this could be a very good way for him to spend his time. And, could even become a motivating reward to be used for behavior modification.
Frea, et al. (2001), tell us that exhibiting extremely challenging behaviors can be improved with some sort of intact communication system which allows the child to express choices and preferences, in all settings.
Cariello (2015) recalls how she started some rudimentary means of communication by posting pictures of her son Jack’s favorite items around the house so he could point to things he needed, but his language was limited to about ten words. In conjunction with his speech therapist and the integrated preschool, Joe and I were doing our best to figure out our enigmatic little boy.
Just as autism varies from person to person over time, as Jack gets older, his autism changes year by year. He was very difficult that spring. In his preschool back in Buffalo he’d started biting and kicking both kids and teachers, and everyone seemed at a loss as to how to control his behavior. At home he’d started to hit both Joe and I, and to get into other mischief.
Hill & Flores (2014) tell us that many children with Autism Spectrum Disorder and/or Developmental Delays cannot or do not speak. Some may even lack the gestures such as pointing, waving, flapping, or finding ways to direct persons to what they want or need. Then when the child demonstrates frustration, it is interpreted as noncompliance or defiant behavior. When all they are trying to do is ‘communicate.
These authors suggest Augmentative or Alternative Communication (AAC) devices such as those you can purchase with buttons to push which are programmed with a word or two. Another form of communication they mention is PECS (Picture Exchange Communication System) either in the low-tech form of pictures in a notebook, or App in an iPad. Both require a somewhat involved learning process with a partner who is learning it too.
< My Thoughts > “…PECS…”
Sonny was taught to use PECS in school. He still has his book and looks at it occasionally for amusement, but the idea of using it to communicate never really ‘happened’ for him. We even tried using ‘real’ pictures instead of the graphic ones the program comes with. What he prefers is an AAC device called a ‘Super Talker’ (you can find versions of these online) with recorded messages (in voice of your choice) on four separate picture grids (drink, eat, cookie, help).
We added another ‘Super Talker’ device with four more pictures – car, McDonald’s, garden, coloring book. He has another small four-grid device for the bathroom (toilet, shower, comb hair, drink). Eventually, one grid had Buzz Lightyear’s voice saying, “I have a laser and I will use it! That covered just about anything, signaling that one of us was getting anxious about something that was or wasn’t happening. Yes, I used it too, when I was being ignored! For beginners, you may want to get one big red button which when pushed says whatever you record. Sonny’s first one said “Cookie!” Sonny (aka ‘Cookie Pie’) soon outgrew it but we hooked it up to a musical toy so when you push ‘Big Red’ the toy or music activates. Of course, the most sophisticated Augmentative or Alternative Communication (AAC) device is the computer. There are endless possibilities there. Get busy, there’s plenty to do to help your child while you wait.
Marks (2012) makes a remarkable discovery – In my senior year of high school, something wonderful happened. A lady by the name of Ellie contacted my mom about ‘facilitated communication’.
Rudy (2016) talks about ‘facilitated communication’. – “Facilitated communication involves a combination of physical and emotional support to an individual who has difficulties with speech and with intentional pointing in unassisted typing.”
While some, like Shermer (2016), says that there are those who believe and are enchanted by “an autistic boy typing (with the assistance of a facilitator) a message on an iPad. He writes, “Now you can hear me. The iPad helps me to see not only my words, but to hold onto my thoughts.”
Note: More about PECS and Facilitated Communication in Unit 7.
REFERENCES: UNIT 3; CHAPTER 2 – SPEECH & LANGUAGE COMMUNICATION
Barnes, E. (2014). Building in Circles: The Best of Autism Mom; eBook Edition.
Bradshaw, J., & Klaiman, C. (2018). Walking Ability is Associated with Social Communication Skills in Infants at High Risk for Autism Spectrum Disorder; Journal of the International Congress of infant Studies; V23:5, p674-691.
Brain Balance Writer (2014). Sensory Meltdown vs. Temper Tantrum; Brain Balance Centers; Retrieved from – https://blog.brainbalancecenters.com/2014/11/sensory-meltdown-vs-temper-tantrum/
Cariello, C. (2015). What Color is Monday? How Autism Changed One Family for the Better; eBook Edition.
Decker, J. (2011). I Wish I Were Engulfed in Flames: My Insane Life Raising Two Boys with Autism; eBook Edition.
Denman, K., Smart, C., et al. (2016). How Families Make Sense of Their Child’s Behavior When on an Autism Assessment & Diagnosis Waiting List; Journal of Autism & Developmental Disorders; V46, p3408-3423.
Disease Control & Prevention CDC Milestone Tracker Checklist, pdf. on Learn the Signs. Act Early. (cdc.gov/MilestoneTracker).
Driver, J. (2011). Struggling with Communication - From the Inside Out; Retrieved online from – Psychology Today.com/
Duan-Young, D. Autism: Why I Love Kids with Autism; eBook Edition.
Frea, W., Arnold, C., et al. (2001). A Demonstration of the Effects of Augmentative Communication on the Extreme Aggressive Behavior of a Child With Autism Within an Integrated Preschool Setting; Journal of Positive Behavior Interventions; V3:4, p194.
Greene, R. (2014). The Explosive Child; Harper Publishers, New York, N.Y.
Hill, D. & Flores, M. (2014). Comparing the Picture Exchange Communication System and the iPad for Communication of Students with ASD & DD; TechTrends, V58:3, p45-53.
Hoecker, J. (2018). Is Baby Sign Language Worthwhile?; Retrieved online from – Mayo Clinic.org/
Kover, S., et al. (2016). Brief Report: Ages of Language Milestones as Predictors of Developmental Trajectories in Young Children with Autism Spectrum Disorder; Journal of Autism Developmental Disorders; V46, p2501-2507.
Marks, S. (2012). Paula’s Journal: Surviving Autism; eBook Edition.
Mayo Clinic Staff Writer (2018). Anatomy of a Temper Tantrum; Retrieved online from – Mayo Clinic.org/
Mukhopadhyay, T. (2011). How Can I Talk If My Lips Don’t Move?: Inside My Autistic Mind; eBooks Edition.
Piven, J. (2015). On the Misapplication of the Broad Autism Phenotype Questionnaire in a Study of Autism; Journal of Autism Developmental Disorders; V44, p2077-2078.
Rudy, L. (2016). Does Facilitated Communication Really Work?; Retrieved online from – https://www.verywell.com/facilitated-communication-and-autism/
Shalom, B., et al. (2006). Normal Psysiological Emotions, but Differences in Expression of Conscious Feelings in Children with High-Functioning Autism. Journal of Autism & Developmental Disorders; V 36:3, p395-400.
Shermer, M. (2016). If “facilitated Communication” is a Canard, Why Teach It?: Facilitated Communication, Autism & Patient’s Rights; Retrieved online from – https://www.scientificamerican.com/
Stagliano, K. & McCarthy, J. (2010). All I Can Handle, and I Am No Mother Teresa: A Life Raising Three Daughters with Autism; eBook Edition.
Stokes, S. (2018). Increasing Expressive Skills for Verbal Children with Autism; National Association of Special Education Teachers; Citation: Written by Susan Stokes under a contract with CESA 7 and funded by a discretionary grant from the Wisconsin Department of Public Instruction. Retrieved online from – https://www.naset.org/index.php?id=2771/
Squaresky, M. (2014). A Spot on the Wall; eBook Edition.
WebMD Contributor (2020). Benefits of Speech Therapy for Autism; Retrieved online from – www.webmd.com/brain/autism/benefits-speech-therapy-autism/
Whiffen, L. (2009). A Child’s Journey Out of Autism: One Family’s Story of Living in Hope and Finding a Cure; eBook Edition.
Whippery, A. (2019). Families & Providers; Outpatient Surgery Magazine; p27-34.
CHAPTER 3 – COGNITION & TEMPERAMENT / PERSONALITY
Knowing the difference between tantrums and meltdowns is the key to helping a child through them. It may also help to get a better idea of the kinds of situations that can be challenging for your child. You can also explore tips on how to deal with noise and other sensitivities.
< My Thoughts > “…challenging for your child.”
Challenging for you too, because the difference between a sensory meltdown and a temper tantrum may not be easy to determine, the first time or two. The problem with trying to unlock a child’s sensory needs is that what may be frightening or even terrifyingly unbearable one time may become stimulating and sensory-seeking to the child or student the next time.
Aggression, violence, and other challenging behavior may really be signs of Sensory Issues. Denman, et al. (2016) say – Families of a child diagnosed with autism can find themselves trying to understand their child’s behavior while on the waiting list for ‘formal diagnosis.’ How this ‘parental making sense’ of behaviors affects parenting in the meantime is important. Confusions can also occur for the children who have insecure attachment patterns as well as sensory impairments.
For instance, parents may have difficulty understanding how a slight change in routine can cause a child to have a sensory ‘meltdown’, in the middle of the street. At the same time, parents may be more concerned about the need to present a ‘positive parenting identity’ to friends, family members, or others who are viewing the ‘middle of the street meltdown’.
< My Thoughts > “…viewing the ‘middle of the street meltdown’.…”
When viewing that ‘middle of the street meltdown’, an uninformed society may be determined they are seeing a ‘bad kid’ or ‘bad parenting’, or both. But, AGAIN, “He’s not giving you a bad time.” “He’s having a bad time.”
Note: More about ‘sensory’ behavior in SENSORY UNIT 4
Barnes (2014) relates this – Our son, who we call the Navigator, and I stopped for lunch at a fast-food restaurant. We made it in okay, and finally to the front of the line. It was lunchtime, crowded, with lots of noisy activity. Navigator, began being unable to process the noisy sensory input. He looked up at me. “Do you need to go outside?” He nodded; his eyes large. We went outside and placed our order there. While we waited, my son explored in detail the mysteries of the asphalt parking lot.
Duan-Young (2014) explains that the sound Aimee let out was like something you’d imagine a wild animal would make. First the bed clothes were ripped off the bed. Next, the mattress came off the bed. Aimee had recently come to live in our group home and this was her way of ‘communicating’.
Aimee was not able to verbally communicate. When she became frustrated, or wanted something and didn’t know how to express herself, she would do the only thing she knew. She would become physically violent and destroy whatever was near her.
From a behavioral analyst’s point of view, every behavior has a function, or intent. One of the ‘mistakes’ parents make when children calm down after a tantrum is ask them “Why did you do that?” “Didn’t I tell you that you’re not supposed to do that?” “What’s wrong with you?”
Greene (2014) gives us a newer approach to understanding and parenting the child who seems to be easily frustrated and frequently inflexible. Here are some of Dr. Greene’s Plan B Steps, when Plan A isn’t working – Step 1 is the Empathy Step and is followed by Step 2, the Identify the Problem Step; and Step 3 is the Invitation Step.
< My Thoughts > “…Dr. Greene’s Plan B Steps…”
My version of adapting Plan B steps would go something like this for a neuro-typical child. But needing more adaptation for a child with autism, yet keeping the ‘empathy’ theme.
Step 1 is the Empathy Step
Parent: I’ve noticed that you’ve been struggling a lot over doing your chores lately. What’s up?
Step 2 is the Identify the Problem Step
Child: It’s too hard.
Parent: Which part’s too hard?
Child: There’s too much.
Step 3 is the Invitation Step
Parent: How about taking some time and writing down the chores you don’t mind doing and the ones you don’t want to do. Maybe we can shorten the list, or change some of your choices.
Dr. Greene asks us to keep in mind that every child is at different stages in their emotional and social development. Sometimes the very bright and more astute children have the most difficulty in life, because they ‘know’ that there are many ‘injustices’ or ‘perceived injustices’ in their world. And, they are considerably unhappy until ‘justice’ is served, so to speak.
< My Thoughts > “…‘perceived injustices’…”
This is especially true of the ‘literal thinking’ autistic children and adults. Beware, ‘perceived injustices’ may be cause for a sudden tremendous tantrum.
Shalom, et al. (2006) states that the participants with autism who could express themselves about feelings stated the following – Mostly they only had ‘conscious’ feelings about things which were ‘pleasant’ versus ‘unpleasant’ or, ‘interesting’ versus ‘boring’
Decker (2013) says sometimes her autistic son Jaxson resembles the devil incarnate. But when he smiles, he lights up a room.
“Stars!” “Stars!” Jaxson insists.
“Stars?” I answer back.
“Stars, yes,”
“Stars?” We went back and forth like that for two minutes. He wanted something from me and if I couldn’t figure out what he wanted, in the next twenty seconds or so, ‘you know what’ would be hitting the fan – or the walls. Biting hitting, screaming, kicking – any or all of the above were imminent.
He was doing his part – he was asking. I just wasn’t equal to the task. I had no idea what ‘stars’ meant in his strange little world.
“Stars!” I could see the urgency bubbling up within him. He tilted his head, thinking a minute, the synapses firing in his special brain. “DS?” he inquired.
“DS? You want your Nintendo DS?” He wanted his game! “DS, please.” What stars had to do with DS I had no idea. But you have to love an autistic kid who can still use the word ‘please’.
< My Thoughts > “Nintendo DS…”
On the Nintendo website they tell us that ‘star coins’ can be earned at all levels of the Nintendo DS game. Could it have been earning ‘star coins’ that Jaxson connected with, as a way to communicate that he wanted to play his Nintendo DS?
And, what was the game’s attraction for Jaxson? Probably, as for many players, the chance to interact with the world through action games without leaving the security of his room. For the autistic child, if it improves eye-hand coordination, and possibly even gives him better spatial orientation, this could be a very good way for him to spend his time. And, could even become a motivating reward to be used for behavior modification.
Frea, et al. (2001), tell us that exhibiting extremely challenging behaviors can be improved with some sort of intact communication system which allows the child to express choices and preferences, in all settings.
Cariello (2015) recalls how she started some rudimentary means of communication by posting pictures of her son Jack’s favorite items around the house so he could point to things he needed, but his language was limited to about ten words. In conjunction with his speech therapist and the integrated preschool, Joe and I were doing our best to figure out our enigmatic little boy.
Just as autism varies from person to person over time, as Jack gets older, his autism changes year by year. He was very difficult that spring. In his preschool back in Buffalo he’d started biting and kicking both kids and teachers, and everyone seemed at a loss as to how to control his behavior. At home he’d started to hit both Joe and I, and to get into other mischief.
Hill & Flores (2014) tell us that many children with Autism Spectrum Disorder and/or Developmental Delays cannot or do not speak. Some may even lack the gestures such as pointing, waving, flapping, or finding ways to direct persons to what they want or need. Then when the child demonstrates frustration, it is interpreted as noncompliance or defiant behavior. When all they are trying to do is ‘communicate.
These authors suggest Augmentative or Alternative Communication (AAC) devices such as those you can purchase with buttons to push which are programmed with a word or two. Another form of communication they mention is PECS (Picture Exchange Communication System) either in the low-tech form of pictures in a notebook, or App in an iPad. Both require a somewhat involved learning process with a partner who is learning it too.
< My Thoughts > “…PECS…”
Sonny was taught to use PECS in school. He still has his book and looks at it occasionally for amusement, but the idea of using it to communicate never really ‘happened’ for him. We even tried using ‘real’ pictures instead of the graphic ones the program comes with. What he prefers is an AAC device called a ‘Super Talker’ (you can find versions of these online) with recorded messages (in voice of your choice) on four separate picture grids (drink, eat, cookie, help).
We added another ‘Super Talker’ device with four more pictures – car, McDonald’s, garden, coloring book. He has another small four-grid device for the bathroom (toilet, shower, comb hair, drink). Eventually, one grid had Buzz Lightyear’s voice saying, “I have a laser and I will use it! That covered just about anything, signaling that one of us was getting anxious about something that was or wasn’t happening. Yes, I used it too, when I was being ignored! For beginners, you may want to get one big red button which when pushed says whatever you record. Sonny’s first one said “Cookie!” Sonny (aka ‘Cookie Pie’) soon outgrew it but we hooked it up to a musical toy so when you push ‘Big Red’ the toy or music activates. Of course, the most sophisticated Augmentative or Alternative Communication (AAC) device is the computer. There are endless possibilities there. Get busy, there’s plenty to do to help your child while you wait.
Marks (2012) makes a remarkable discovery – In my senior year of high school, something wonderful happened. A lady by the name of Ellie contacted my mom about ‘facilitated communication’.
Rudy (2016) talks about ‘facilitated communication’. – “Facilitated communication involves a combination of physical and emotional support to an individual who has difficulties with speech and with intentional pointing in unassisted typing.”
While some, like Shermer (2016), says that there are those who believe and are enchanted by “an autistic boy typing (with the assistance of a facilitator) a message on an iPad. He writes, “Now you can hear me. The iPad helps me to see not only my words, but to hold onto my thoughts.”
Note: More about PECS and Facilitated Communication in Unit 7.
REFERENCES: UNIT 3; CHAPTER 2 – SPEECH & LANGUAGE COMMUNICATION
Barnes, E. (2014). Building in Circles: The Best of Autism Mom; eBook Edition.
Bradshaw, J., & Klaiman, C. (2018). Walking Ability is Associated with Social Communication Skills in Infants at High Risk for Autism Spectrum Disorder; Journal of the International Congress of infant Studies; V23:5, p674-691.
Brain Balance Writer (2014). Sensory Meltdown vs. Temper Tantrum; Brain Balance Centers; Retrieved from – https://blog.brainbalancecenters.com/2014/11/sensory-meltdown-vs-temper-tantrum/
Cariello, C. (2015). What Color is Monday? How Autism Changed One Family for the Better; eBook Edition.
Decker, J. (2011). I Wish I Were Engulfed in Flames: My Insane Life Raising Two Boys with Autism; eBook Edition.
Denman, K., Smart, C., et al. (2016). How Families Make Sense of Their Child’s Behavior When on an Autism Assessment & Diagnosis Waiting List; Journal of Autism & Developmental Disorders; V46, p3408-3423.
Disease Control & Prevention CDC Milestone Tracker Checklist, pdf. on Learn the Signs. Act Early. (cdc.gov/MilestoneTracker).
Driver, J. (2011). Struggling with Communication - From the Inside Out; Retrieved online from – Psychology Today.com/
Duan-Young, D. Autism: Why I Love Kids with Autism; eBook Edition.
Frea, W., Arnold, C., et al. (2001). A Demonstration of the Effects of Augmentative Communication on the Extreme Aggressive Behavior of a Child With Autism Within an Integrated Preschool Setting; Journal of Positive Behavior Interventions; V3:4, p194.
Greene, R. (2014). The Explosive Child; Harper Publishers, New York, N.Y.
Hill, D. & Flores, M. (2014). Comparing the Picture Exchange Communication System and the iPad for Communication of Students with ASD & DD; TechTrends, V58:3, p45-53.
Hoecker, J. (2018). Is Baby Sign Language Worthwhile?; Retrieved online from – Mayo Clinic.org/
Kover, S., et al. (2016). Brief Report: Ages of Language Milestones as Predictors of Developmental Trajectories in Young Children with Autism Spectrum Disorder; Journal of Autism Developmental Disorders; V46, p2501-2507.
Marks, S. (2012). Paula’s Journal: Surviving Autism; eBook Edition.
Mayo Clinic Staff Writer (2018). Anatomy of a Temper Tantrum; Retrieved online from – Mayo Clinic.org/
Mukhopadhyay, T. (2011). How Can I Talk If My Lips Don’t Move?: Inside My Autistic Mind; eBooks Edition.
Piven, J. (2015). On the Misapplication of the Broad Autism Phenotype Questionnaire in a Study of Autism; Journal of Autism Developmental Disorders; V44, p2077-2078.
Rudy, L. (2016). Does Facilitated Communication Really Work?; Retrieved online from – https://www.verywell.com/facilitated-communication-and-autism/
Shalom, B., et al. (2006). Normal Psysiological Emotions, but Differences in Expression of Conscious Feelings in Children with High-Functioning Autism. Journal of Autism & Developmental Disorders; V 36:3, p395-400.
Shermer, M. (2016). If “facilitated Communication” is a Canard, Why Teach It?: Facilitated Communication, Autism & Patient’s Rights; Retrieved online from – https://www.scientificamerican.com/
Stagliano, K. & McCarthy, J. (2010). All I Can Handle, and I Am No Mother Teresa: A Life Raising Three Daughters with Autism; eBook Edition.
Stokes, S. (2018). Increasing Expressive Skills for Verbal Children with Autism; National Association of Special Education Teachers; Citation: Written by Susan Stokes under a contract with CESA 7 and funded by a discretionary grant from the Wisconsin Department of Public Instruction. Retrieved online from – https://www.naset.org/index.php?id=2771/
Squaresky, M. (2014). A Spot on the Wall; eBook Edition.
WebMD Contributor (2020). Benefits of Speech Therapy for Autism; Retrieved online from – www.webmd.com/brain/autism/benefits-speech-therapy-autism/
Whiffen, L. (2009). A Child’s Journey Out of Autism: One Family’s Story of Living in Hope and Finding a Cure; eBook Edition.
Whippery, A. (2019). Families & Providers; Outpatient Surgery Magazine; p27-34.
CHAPTER 3 – COGNITION & TEMPERAMENT / PERSONALITY
COGNITION –
Case-Lo (2014) claims that the causes of autism are not entirely known, but are likely a mixture of genetic and environmental factors. Recent studies suggest that the symptoms of autism may be the result of ‘patches of disorganization’ in the ‘neocortex’ of the brain.
Cherry (2020) considers ‘cognition’ the mental process requiring knowledge & understanding of what one is experiencing in their environment. Shows ability to use working memory, make judgments, reason, problem solve & make decisions. In the ordinary world, ‘cognition’ or the ability of the child to make sense of their world by asking and answering questions, appropriately. By participating in a back-and-forth conversation, appropriately and by learning through active listening and paying attention. Another way to show ‘cognition’ is by showing ability to use short-term and long-term memory; as well as being able to understand the world from someone else’s perspective.
Cohen (2011) But there’s so much I read about autism that doesn’t fit Ezra. He had normal eye contact; at least once he is comfortable with someone. He initiates peek-a-boo and chasing games. He plays normally with most toys, albeit sometimes in rigid ways.
This may be one of the first concerns that parents have, that some things seem to ‘fit’ while others don’t. Most studies show that with early identification and intervention, children with autism, both verbal and non-verbal, have made cognitive gains with help. These gains can be made by helping the child expand and explore experiences in their natural setting (at home and community) while you wait.
< My Thoughts > “While you wait…”
While you're waiting for the world of doctor’s appointments, consultations, and program possibilities to open up for you, you might try some of these suggestions.
The CDC Milestone Tracker suggests some of the following activities to do with your child:
2 – months:
Retrieved online from – CDC Milestone Tracker Checklist, pdf. on Learn the Signs. Act Early. (cdc.gov/MilestoneTracker).
Cariello (2015) talks about her six-year-old son Jack – The doctor recommended neurophysychological testing to get an accurate picture of exactly how Jack thinks and reacts in certain situations. Much of Jack’s issues, it turns out, are related to sensory integration and his own internal regulation. He struggles with regulation, cognitive flexibility, working memory and processing, and auditory and visual complexity.
As a ‘literal’ thinker he has trouble with cognitive flexibility and ‘theory of mind’. An aspect of social cognition, ‘theory of mind’ is the ability to understand that others have beliefs, opinions, and feelings different than your own. Jack however, thinks everyone sees and feels and likes the same things he does. Literal boys like my Jack, are boys who start looking around wildly for giraffes when their mother announces that the box store parking lot is a zoo!
< My Thoughts > “…the same things he does.”
‘Theory of Mind’ is thinking that everyone is having the same ‘sensory experience’ that you are. How do you increase a person’s ‘theory of mind’ and help them understand that others think and feel differently?
With the help of our psychologist, we created a strategy to increase Jack’s ability in each of the identified areas:
Jack’s limited working memory results in significant communication challenges. In his mind words are as slippery as falling snowflakes, and as quickly as he grabs hold of one idea, another one slides out of his cerebral grasp.
When he’s asked a question it’s as though Jack has to mentally bend down and retrieve that one idea out of many, re-examine it, and figure out if it’s what he needs. It takes him a while to answer.
< My Thoughts > “When he’s asked a question…”
When he’s asked a question it’s as though he has to mentally bend down and retrieve that one idea out of many, re-examine it, and figure out if it’s what he needs. It takes him a while to answer. This so perfectly states what I think that many children with autism go through. In fact, when hearing the words ‘developmental delay’, people often think that the child has mental processing issues, or thinking delays. When in fact it means that they are ‘delayed’ in meeting their traditional developmental milestones. Such as, taking time to respond to mother’s voice, time to turn his head to sounds, time to babble, and so forth.
Kuzma (2012) believes you can teach ‘perspective-taking’ skills. Around 2-3 years old a child begins to gain the understanding that each person is experiencing different things. And, that each person’s experiences are different. Saying that at this early stage, young children often confuse their own perspective with that of others. They are working through understanding how they have accidently caused another child to cry. A child can be helped to problem-solve, to make the situation better for everyone else, and to talk about how emotions are oftentimes the cause of behaviors. Sometimes they can learn from the modeling of others. Sometimes, from the characters in a book.
< My Thoughts > “…characters in a book.”
One group of characters which come to mind are those in the story of The Three Little Pigs. Each character, the three pigs and the wolf, have a different perspective as the story of house-building unfolds. Engaging the child in discovery and awareness of each character’s feelings, emotions, actions, attitude, and of course perspective. Woven into this lesson would hopefully be an emerging understanding of delayed gratification, evaluation of self and others, of what persons value and respect, and of experiential connections.
Chess & Thomas (1995) communicate that most children and adults master the trials of daily living while others fail to meet the same demands at home, at school, with peers and at work. So, professionals are trying to understand why we have such behavioral differences. And to determine interventions that will eliminate, or at least reduce, problems in functioning. Recently, there has been renewed interest in understanding a child's temperament in order to help us treat a range of behavior and conduct problems. They believe that temperament predictability can even help to prevent the onset of certain undesirable behaviors.
< My Thoughts > “…prevent the onset…”
There are many stories of families going bankrupt while trying to ‘cure’ or reduce the effects of their child’s autism. So much must be considered before committing to an intervention program. The CDC believes that ‘early intervention’ is the key to a child becoming as productive as possible, learning daily living skills, and living a fulfilling life. But, the careful consideration as to the ‘limits’ and ‘expectations’ of autism interventions is strongly suggested, for the wellbeing of all family members. While you wait, investigate.
Cohen (2011) says – Ezra is almost two years old, but he still isn’t consistent with sign language and he has no words, so I think about pursuing outside opinions. I call Early Intervention first, a state program that is mandated by federal law.
“What sorts of things are you concerned about?” the coordinator asks me on the phone. “I’m not concerned,” I say. I’m aware that I’m pacing as we talk. “But I know he’s supposed to have a few words by now, and I figure speech therapy could help.”
“So, he isn’t talking yet. How old is he, again?” I tell her, not wanting to. “He’s twenty-one months.” “Any other concerns?”
His poor eating. No pointing. Crying when songs end. He cries in terrible despair if someone stops singing his favorite songs.
< My Thoughts > “Crying when songs end.”
Our Sonny cannot tolerate when something ends, whether it’s a song or a DVD. So, we make every effort to keep his favorites available on a ‘loop’. Somehow in the same vein, in the ‘Sonny Ending/Empty is Time to Panic Category,’ this includes empty glasses, empty cups, empty food dishes, and empty or partially-filled cereal boxes, containers in the refrigerator which are getting low. He doesn’t even have to be able to see inside, he knows how long it’s been in there, how many times it’s been used, and probably what the ‘use by’ date is. This phobia-like behavior has become less over the years. Apparently, he finally is beginning to trust us to refill and replenish before the disappearance becomes too crushing for him.
Case-Lo (2014) claims that the causes of autism are not entirely known, but are likely a mixture of genetic and environmental factors. Recent studies suggest that the symptoms of autism may be the result of ‘patches of disorganization’ in the ‘neocortex’ of the brain.
Cherry (2020) considers ‘cognition’ the mental process requiring knowledge & understanding of what one is experiencing in their environment. Shows ability to use working memory, make judgments, reason, problem solve & make decisions. In the ordinary world, ‘cognition’ or the ability of the child to make sense of their world by asking and answering questions, appropriately. By participating in a back-and-forth conversation, appropriately and by learning through active listening and paying attention. Another way to show ‘cognition’ is by showing ability to use short-term and long-term memory; as well as being able to understand the world from someone else’s perspective.
Cohen (2011) But there’s so much I read about autism that doesn’t fit Ezra. He had normal eye contact; at least once he is comfortable with someone. He initiates peek-a-boo and chasing games. He plays normally with most toys, albeit sometimes in rigid ways.
This may be one of the first concerns that parents have, that some things seem to ‘fit’ while others don’t. Most studies show that with early identification and intervention, children with autism, both verbal and non-verbal, have made cognitive gains with help. These gains can be made by helping the child expand and explore experiences in their natural setting (at home and community) while you wait.
< My Thoughts > “While you wait…”
While you're waiting for the world of doctor’s appointments, consultations, and program possibilities to open up for you, you might try some of these suggestions.
The CDC Milestone Tracker suggests some of the following activities to do with your child:
2 – months:
- Talk, read, sing to your baby
- Encourage your child to play peek-a-boo
- Hold a toy or rattle so baby can reach for it
- Place toys near your child so s/he can reach or kick them
- Provide opportunities for your child to safely explore his/her surroundings
- When your baby looks at something, point to it and talk about it.
- When s/he drops something, pick it up and give back. Teaches cause/effect
- Teach more cause/effect by rolling a ball back & forth saying “My turn” … “Your turn”
- Say what you think your baby’s feeling… “Are you hungry?” “Are you sleepy?”
- Try to stick to an established daily & nightly routine
- Help your child follow simple directions “Pick up toy”
- Show your child how to point to what s/he wants, using pointer finger
- Build on what your child is trying to say… “Yes, that’s a big blue truck.”
- Help your child know what ordinary things are… spoon, cup, toy…
- Help your child point to body parts
- Help your child follow simple commands
- Help your child learn & complete rhymes
- Teach your child to build a tower with more than 2 blocks
- Help your child sort by colors & numbers
- Give your child the opportunity to work toys with buttons, levers, & moving parts
- Give your child the opportunity to work 2 – 4 piece puzzles
- Give your child the opportunity to copy shapes with a pencil or crayon
- Give your child the opportunity to say first & last name & phone number
- Give your child the opportunity to sing songs from memory
- Give your child the opportunity to tell stories
- Give your child the opportunity to learn name, parent’s name, address & phone number
- Give your child the opportunity to have a ‘play’ date
- Give your child the opportunity to explore his or her interests
Retrieved online from – CDC Milestone Tracker Checklist, pdf. on Learn the Signs. Act Early. (cdc.gov/MilestoneTracker).
Cariello (2015) talks about her six-year-old son Jack – The doctor recommended neurophysychological testing to get an accurate picture of exactly how Jack thinks and reacts in certain situations. Much of Jack’s issues, it turns out, are related to sensory integration and his own internal regulation. He struggles with regulation, cognitive flexibility, working memory and processing, and auditory and visual complexity.
As a ‘literal’ thinker he has trouble with cognitive flexibility and ‘theory of mind’. An aspect of social cognition, ‘theory of mind’ is the ability to understand that others have beliefs, opinions, and feelings different than your own. Jack however, thinks everyone sees and feels and likes the same things he does. Literal boys like my Jack, are boys who start looking around wildly for giraffes when their mother announces that the box store parking lot is a zoo!
< My Thoughts > “…the same things he does.”
‘Theory of Mind’ is thinking that everyone is having the same ‘sensory experience’ that you are. How do you increase a person’s ‘theory of mind’ and help them understand that others think and feel differently?
With the help of our psychologist, we created a strategy to increase Jack’s ability in each of the identified areas:
- Self-regulation
- Communication
- Cognitive ability
Jack’s limited working memory results in significant communication challenges. In his mind words are as slippery as falling snowflakes, and as quickly as he grabs hold of one idea, another one slides out of his cerebral grasp.
When he’s asked a question it’s as though Jack has to mentally bend down and retrieve that one idea out of many, re-examine it, and figure out if it’s what he needs. It takes him a while to answer.
< My Thoughts > “When he’s asked a question…”
When he’s asked a question it’s as though he has to mentally bend down and retrieve that one idea out of many, re-examine it, and figure out if it’s what he needs. It takes him a while to answer. This so perfectly states what I think that many children with autism go through. In fact, when hearing the words ‘developmental delay’, people often think that the child has mental processing issues, or thinking delays. When in fact it means that they are ‘delayed’ in meeting their traditional developmental milestones. Such as, taking time to respond to mother’s voice, time to turn his head to sounds, time to babble, and so forth.
Kuzma (2012) believes you can teach ‘perspective-taking’ skills. Around 2-3 years old a child begins to gain the understanding that each person is experiencing different things. And, that each person’s experiences are different. Saying that at this early stage, young children often confuse their own perspective with that of others. They are working through understanding how they have accidently caused another child to cry. A child can be helped to problem-solve, to make the situation better for everyone else, and to talk about how emotions are oftentimes the cause of behaviors. Sometimes they can learn from the modeling of others. Sometimes, from the characters in a book.
< My Thoughts > “…characters in a book.”
One group of characters which come to mind are those in the story of The Three Little Pigs. Each character, the three pigs and the wolf, have a different perspective as the story of house-building unfolds. Engaging the child in discovery and awareness of each character’s feelings, emotions, actions, attitude, and of course perspective. Woven into this lesson would hopefully be an emerging understanding of delayed gratification, evaluation of self and others, of what persons value and respect, and of experiential connections.
Chess & Thomas (1995) communicate that most children and adults master the trials of daily living while others fail to meet the same demands at home, at school, with peers and at work. So, professionals are trying to understand why we have such behavioral differences. And to determine interventions that will eliminate, or at least reduce, problems in functioning. Recently, there has been renewed interest in understanding a child's temperament in order to help us treat a range of behavior and conduct problems. They believe that temperament predictability can even help to prevent the onset of certain undesirable behaviors.
< My Thoughts > “…prevent the onset…”
There are many stories of families going bankrupt while trying to ‘cure’ or reduce the effects of their child’s autism. So much must be considered before committing to an intervention program. The CDC believes that ‘early intervention’ is the key to a child becoming as productive as possible, learning daily living skills, and living a fulfilling life. But, the careful consideration as to the ‘limits’ and ‘expectations’ of autism interventions is strongly suggested, for the wellbeing of all family members. While you wait, investigate.
Cohen (2011) says – Ezra is almost two years old, but he still isn’t consistent with sign language and he has no words, so I think about pursuing outside opinions. I call Early Intervention first, a state program that is mandated by federal law.
“What sorts of things are you concerned about?” the coordinator asks me on the phone. “I’m not concerned,” I say. I’m aware that I’m pacing as we talk. “But I know he’s supposed to have a few words by now, and I figure speech therapy could help.”
“So, he isn’t talking yet. How old is he, again?” I tell her, not wanting to. “He’s twenty-one months.” “Any other concerns?”
His poor eating. No pointing. Crying when songs end. He cries in terrible despair if someone stops singing his favorite songs.
< My Thoughts > “Crying when songs end.”
Our Sonny cannot tolerate when something ends, whether it’s a song or a DVD. So, we make every effort to keep his favorites available on a ‘loop’. Somehow in the same vein, in the ‘Sonny Ending/Empty is Time to Panic Category,’ this includes empty glasses, empty cups, empty food dishes, and empty or partially-filled cereal boxes, containers in the refrigerator which are getting low. He doesn’t even have to be able to see inside, he knows how long it’s been in there, how many times it’s been used, and probably what the ‘use by’ date is. This phobia-like behavior has become less over the years. Apparently, he finally is beginning to trust us to refill and replenish before the disappearance becomes too crushing for him.
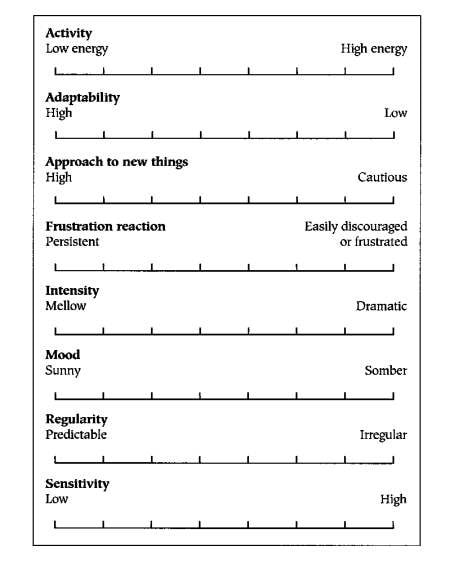
Staff Writer (2019) states that physicians have found that several factors combine with temperament to shape
personality throughout childhood and adult life. They are –
They go on to say that the interaction between clinicians, teachers, and those in your child’s learning environment need to be a ‘good fit’, in order for everyone to become successful. An example they cite is that if your daughter has a ‘low stimulation’ threshold, therapists may make you aware that she could be irritated by wearing scratchy clothing. She may be irritable about wearing something new, even new socks, and you wouldn’t necessarily understand why.
< My Thoughts > “…new socks…”
Some children always want to wear their socks or stockings ‘inside-out’ because they are not so scratchy that way. Label-free and specialty clothing can be purchased online.
Hunter (2015) has said that she was socialized within the paradigm of adult power and control. But as a parent herself, wanted to be respective of her child. Yet she wished to gain her children’s compliance while still putting forth her parental perspective. ”I wanted my children to accept changes while managing to keep calm. My need was to get them to comply without argument, in the moment. I wanted them to see what needed to done, and do it.”
< My Thoughts > “…comply without argument…”
As a parent, and as an educator, how many times when operating on my last nerve, did I want to yell – “Just DO IT!!!” But no, it’s all about motivation, salesman or saleswomanship, and velvet gloves; as Hunter explains.
Hunter continues that meantime children are learning how to use power over others. How what they want doesn’t matter. But when we take time to understand what they are feeling, that we are trying to respect and trust them, they know we care about them. They learn that it feels good to be cared for in that way.
She says that when our needs are in conflict with the child’s needs, it often causes us to ‘react’ instead of ‘reframing’ to meet everyone’s needs. “I need your attention at any cost!” may be what the toddler is thinking. Whether s/he has your attention through good or bad behavior is irrelevant to them.
Another ‘perspective’ problem is that toddlers really believe that you should be able to read their mind. When your angel asks for a cup of water and you deliver it in the wrong cup and without a straw, why are you surprised when the result is a tantrum?
< My Thoughts > “…a cup of water…”
You should ‘know’ what they expect to see when they ask for a cup of water. Right? Just one of the many ways in which ‘knowing your child’ can be fundamental in making the ‘right’ choices.
A person's executive functioning skills make it possible for one to live, work, and learn with an appropriate level of independence and competence for one’s age. This brings up the point of limited communication. Children don’t often have the words or vocabulary to match their thoughts or needs.
< My Thoughts > “…limited communication.”
For children who seem to be always anxious and somewhat impatient by nature, trying early ‘baby’ signing may be helpful. Simple communication is often the key which prevents communication breakdown and unwanted tantrums.
The following list of ‘executive functioning’ allows us to access information, think about solutions, and implement those solutions. Because executive functioning is a theory and not a fully defined, documented, and verified idea, professionals have differing opinions about what mental processes are involved.
Normal ‘executive functioning’ may involve abilities such as:
< My Thoughts > “…without mindful awareness.”
While our brain’s executive functioning goes on throughout life without mindful awareness, it seems to become less visible during the ‘teenage’ years. The ‘teen brain’ is one of wonder.
NIH Staff Writer (2020) – Seven things to know about the ‘teen brain’ –
1. The brain reaches its biggest size in early adolescence. For girls this happens at 11 years of age; for boys its 14 years of age.
2. The brain continues to mature after it has stopped growing. The prefrontal cortex is one of the last regions to mature. This is responsible for skills like planning, prioritizing, and controlling impulses.
3. The teen brain is ready to learn and adapt. It has lots of plasticity, likes creative activities and changes and learns according to experiences and the environment.
4. Many mental disorders may begin to appear during adolescence. The mental disorders which can emerge during this period are – schizophrenia, anxiety disorder, depression, bipolar, and eating disorders.
5. Teen brains may be more vulnerable to stress as they respond differently than adults. Learning ‘meditation and mindfulness’ might help teens cope to reduce stress.
6. Teens need more sleep than children or adults. The sleep hormone levels of Melatonin shift and may cause teens to stay up late and struggle with getting up in the morning.
7. The teen brain is resilient, although vulnerable during this phase of development. Usually, teens get through this period to go on to become healthy adults.
< My Thoughts > “…phase of development.”
What happens when ‘cognition’, the mental process requiring knowledge & understanding of what one is experiencing in their environment, and the ‘phase of development’ of the teenage brain, and the lifelong cognition issues of an individual with autism COLLIDE? Added to this, the ordinary physical and emotional problems one experiences during adolescence can become overwhelming for any parent to deal with.
Ballan & Freyer (2017) found that some may consider the adolescent with ASD as a perpetual child, failing to acknowledge emerging sexual needs and issues. While a child’s public display of affection may seem appropriate for his/her developmental age, it could be disturbing, due to a mature physical appearance. Often ‘sexual education’ is provided only after the person demonstrated problematic sexual behavior. They found that with the help of Mental Health professionals, persons with autism could learn to cope with the physical, social, and emotional transitions of puberty, before the chance of issues arising. Some of the therapies discussed in the study were Cognitive Behavioral Therapy (CBT), Applied Behavior Analysis (ABA), and the use of Social Stories.
Note: More about Cognitive-Behavioral Therapy (CBT); more about Sexual Behavior in UNIT 4, Ch. 2; & Applied Behavior Analysis (ABA) in UNIT 7-2 on Complementary and Alternative Medicine (CAMs)
< My Thoughts > “…learn to cope…”
The degree to which an autistic child, adolescent, and/or adult will respond to helpful therapy depends upon the developmental levels and the cognitive abilities of the person with autism. And, most therapy can only provide ways to lessen symptoms, or to learn how to cope with sensory needs; as the ‘core’ symptoms of autism seem to be lifelong.
Davide-Rivera (2013) discusses how unchanging routines played a part in her life. For instance, a Fall scene played itself over and over again. The leaves dried up, snow fell, flowers bloomed, and days changed, but the routine never changed.
I don’t like interruption. If I am interrupted it is impossible to resume what I was doing without delay. My brain needs time to make the switch.
When I am writing, and the phone rings, or the kids interrupt, it takes a few minutes to even process what is going on. Mostly I am angered by the interruption, even today as an adult.
Freeman & Muraven (2010) tell us that ‘task interruption’ is especially harmful to a person with limited self-resources, and particularly so if they are close to the completion of that task, or it is a task that they are enjoying.
The interruption can be just a trivial irritation, if the person didn’t like the task, to becoming angry and impulsive. This has to do with self-control and self-regulation which could bring on frustration with stopping and starting an activity. The more often it occurs, the more negative the person’s response is to being interrupted.
Jones (2013) candidly admits, I often find myself unable to do something I could easily do the day before.
< My Thoughts > “…something I could do the day before.”
Parents and teachers are often completely puzzled by this kind of event. We make all kinds of excuses… ‘having a bad day’. ‘Must have forgotten from one day to the next’. ‘Not feeling cooperative today’. And, so on. No, you don’t have the correct answer. Oh sure, sometimes there could be any or all of those reasons, but probably it’s because the neuro-passages are not connecting at that moment in time.
Teachers may even get a note from the parent – “She seems to have forgotten how to pull up her pants. Are you still working on that at school? We have to be consistent with her you know.” And, I’m certain the parents have had a note with the reverse message from school. “Are you still working on that at home? We have to be consistent with her you know.”
Some days our brains are firing on all cylinders and some days they simply are not. You have probably experienced this yourself. We ‘neuro-typicals’ just go get a latte and move on. People with autism can’t seem to make just drinking a latte work for them.
Sohn (2020) says that even today, doctors often conflate autism and intellectual disability. That the biological distinction between them can be murky. And, that scientific progress depends on knowing where the conditions intersect – and part ways. In the clinic, though, clearer diagnosis would lead people to services more appropriate for them. On the other hand, they also know what kinds of doors open to those with an autism diagnosis, so they may err on the side of autism if they are not sure.
< My Thoughts > “…err on the side of autism…”
This could lead to a misdiagnosis sending children on another intervention trajectory altogether. Disappointing, when early and correct diagnoses are so important, to say nothing of the private and insurance monies which may be spent in error.
Nordahl (2018) talks on YouTube about a research study looking at 112 boys and 27 girls with autism between age three and five years, as well as a control sample of 53 boys and 29 girls without autism. Using a process called diffusion tensor imaging, the researchers looked at the corpus callosum—the largest neural fiber bundle in the brain—in the young kids. Prior research has shown differences in that area of the brain among people with autism. They found that the organization of these fibers was different in boys compared to girls, especially in the frontal lobes which play a role in executive functions.
Buxhoeveden, et al. (2006) believe that the frontal lobe is involved with the kind of higher-order cognitive, language and socio-emotional functions that are impaired in autism. The scarcity of developmental anatomical evidence requires the necessity of MRI studies in young children, 2 – 4 years old. With further of these studies, they are finding that failure of the cortical area to grow has resulted in narrow vertical ‘microorganization’; thus, reducing the child’s ability to generalize. This brain feature, it is suggested, enhances specialization abilities. The failure of the frontal cortex to continue growing suggests the normal process of brain growth has been stunted.
< My Thoughts > “…enhances specialization and reduces generalization…”
‘Enhanced specialization’ and ‘reduced generalization’ becomes concerning to most parents. Their rigid behavior becomes annoying and worrisome. Let’s say that their child becomes focused/specialized in one area. That area may be the distinct shape, feature, and color of a certain dinosaur. Or, the features of car license plates. Perhaps they spend the whole day lining up cars by size, model, or color. But when that same child is asked to’ generalize’ a similar action in a ‘sorting’ activity, they have no idea how to do it.
According to Bogdashina & Casanova (2016), deficits in planning, organizing and monitoring progress towards a goal often prevents one from taking a flexible approach to problem-solving. “Poor Executive Function can easily account for the lack of thinking flexibility and explains the rigidity of thinking exhibited by autistic people, including starting and finishing tasks which include all of the above.”
< My Thoughts > “…which include all of the above.”
One of the reasons that an autism diagnosis may come during the beginning school years could be due to ‘all of the above’. When the classroom demands which are made on a child extend beyond his or her executive functioning capabilities, then the ‘red flags’ go up, causing parents and teachers to become concerned.
Davide-Rivera (2013) – As a child, I was carefree – happy, as I knew happy to be at the time. But when I grew into a young woman life got messy, and continued to come unraveled as time went on. I had difficulty making friends, raising children, and communicating with my husband largely due to my autism.
It took 38 years for me to be diagnosed with Asperger’s Syndrome (AS), as a form of high functioning autism – 38 years of confusing experiences.
One of the first things that I learned about my Asperger’s diagnosis is that there are three core ‘cognition’ deficits which accompany this condition – the lack of theory of mind, executive dysfunction, and weak central coherence.
Mandy (2013) makes it known that diagnostic tests often miss girls, especially if they are of average intelligence. And, if females are diagnosed, it is much later than their male equivalents. One reason is that repetitive behaviors present in more socially normative ways, as the symptoms of personality or anxiety disorders. He also explains that the current diagnostic assessments are based on the extensive study of ‘boys’ with autism.
< My Thoughts > “…tests often miss girls…”
When my special education classroom consisted mainly of middle-school boys, a student came to me from out of state, in the middle of the semester. She didn’t have an Individualized Education Program (IEP) and was placed with me until more data about an appropriate placement could be obtained. The experienced social worker assigned to our school suspected that this student had learning disabilities, had missed a lot of school, and/or could have an emotional disorder. Eventually, against the parent’s hopes, we convinced them that she required testing before we could place her into the mainstream general education classes. By the end of that school year, she was diagnosed as having Asperger’s Syndrome (AS), with possible passive-aggressive behavior/personality disorder. And, because her family moved around a lot, she had missed critical parts of her early foundational education.
Nordahl (2018) knows that the few studies of girls with autism which have been done have shown that girls can even be affected more severely than boys. They recommended that more girls be found and recruited for studies, intervention, and treatment.
REFERENCES: UNIT 3; CHAPTER 3 – COGNITION
Ballan, M. & Freyer, M. (2017). Autism Spectrum Disorder, Adolescence, & Sexuality Education: Suggested Interventions for Mental Health Professionals; Sexual & Disability Journal; V35, p261-273.
Bogdashina, O., & Casanova, M. (2016). Sensory Perceptual Issues in Autism & Asperger Syndrome; 2nd Edition, eBook.
Buxhoeveden, D., Semendeferi, J., et al. (2006). Reduced minicolumns in the Frontal Cortex of Patients with Autism; Neuropathology & Applied Neurobiology; V32, p483-491.
Cariello, C. (2015). What Color is Monday? How Autism Changed One Family for the Better; eBook Edition.
Case-Lo, C. (2014). What’s the Connection Between Autism & Inflammation?; Retrieved online from –
healthline.com/health-news/connection-between-inflammation-and-autism/
Cherry, K. (2020). What Is Cognition?; Retrieved online from – https://www.verywellmind.com/what-is-cognition-2794982/
Chess, S. & Thomas, A. (1995). Keep Your Child's Temperament In Mind When Analyzing Problems & Solutions; Brown University Child & Adolescent Behavior Letter; V11:6.
Cohen, K. (2011). Seeing Ezra: A Mother’s Story of Autism, Unconditional Love, and the Meaning of Normal; eBook 2011 Edition.
Davide-Rivera, J. (2013). Twirling Naked in the Streets and No One Noticed: Growing Up with Autism; eBook Edition.
Freeman, N., & Muraven, M. (2010). Don’t interrupt me! Task interruption depletes one’s limited resources; Motivation & Emotion V34:3, p. 230-241.
Hunter, W. (2015). How Children Learn to See Someone Else’s Perspective; Retrieved online from –https:/parentingforsocialchange.com/perspective-taking-html/
Jones, S. (2013). No You Don’t – Essays from an Unstrange Mind; eBook Edition.
Kuzma, J. (2012). Perspective-taking Skills; World Press. Also reprinted in https://www.speechand languagekids.com/
Mandy, W. (2013). DSM-5 May Better Serve Girls with Autism; Spectrum Opinion Viewpoint; May Issue.
NIH Staff Writer (2020). The Teen Brain: 7 Things to Know; U.S. National Institutes of Health; Retrieved online from – https://www.nimh.nih.gov/health/publications/
Nordahl, C. (2018). Brains Wired Differently; YouTube, Autism Research; Retrieved online from – https://neuroscience.ucdavis.edu/people/christine-nordahl/
Sohn, E. (2020). The Blurred Line Between Autism & Intellectual Disability; Autism Research News. Retrieved online from – https://www.spectrumnews.org/author/emilysohn
Staff Writer (2019). Temperament, the Preventative Ounce; Retrieved online from – preventativeoz.org/
TEMPERAMENT / PERSONALITY –
personality throughout childhood and adult life. They are –
- Cognition – Does s/he understand the purpose of what’s going on around them?
- Self-awareness – Does s/he understand that there is a world outside themselves?
- Motivation – What are the child’s motivators? (Probably the things s/he fixates, focuses, or perseverates on.)
They go on to say that the interaction between clinicians, teachers, and those in your child’s learning environment need to be a ‘good fit’, in order for everyone to become successful. An example they cite is that if your daughter has a ‘low stimulation’ threshold, therapists may make you aware that she could be irritated by wearing scratchy clothing. She may be irritable about wearing something new, even new socks, and you wouldn’t necessarily understand why.
< My Thoughts > “…new socks…”
Some children always want to wear their socks or stockings ‘inside-out’ because they are not so scratchy that way. Label-free and specialty clothing can be purchased online.
Hunter (2015) has said that she was socialized within the paradigm of adult power and control. But as a parent herself, wanted to be respective of her child. Yet she wished to gain her children’s compliance while still putting forth her parental perspective. ”I wanted my children to accept changes while managing to keep calm. My need was to get them to comply without argument, in the moment. I wanted them to see what needed to done, and do it.”
< My Thoughts > “…comply without argument…”
As a parent, and as an educator, how many times when operating on my last nerve, did I want to yell – “Just DO IT!!!” But no, it’s all about motivation, salesman or saleswomanship, and velvet gloves; as Hunter explains.
Hunter continues that meantime children are learning how to use power over others. How what they want doesn’t matter. But when we take time to understand what they are feeling, that we are trying to respect and trust them, they know we care about them. They learn that it feels good to be cared for in that way.
She says that when our needs are in conflict with the child’s needs, it often causes us to ‘react’ instead of ‘reframing’ to meet everyone’s needs. “I need your attention at any cost!” may be what the toddler is thinking. Whether s/he has your attention through good or bad behavior is irrelevant to them.
Another ‘perspective’ problem is that toddlers really believe that you should be able to read their mind. When your angel asks for a cup of water and you deliver it in the wrong cup and without a straw, why are you surprised when the result is a tantrum?
< My Thoughts > “…a cup of water…”
You should ‘know’ what they expect to see when they ask for a cup of water. Right? Just one of the many ways in which ‘knowing your child’ can be fundamental in making the ‘right’ choices.
A person's executive functioning skills make it possible for one to live, work, and learn with an appropriate level of independence and competence for one’s age. This brings up the point of limited communication. Children don’t often have the words or vocabulary to match their thoughts or needs.
< My Thoughts > “…limited communication.”
For children who seem to be always anxious and somewhat impatient by nature, trying early ‘baby’ signing may be helpful. Simple communication is often the key which prevents communication breakdown and unwanted tantrums.
The following list of ‘executive functioning’ allows us to access information, think about solutions, and implement those solutions. Because executive functioning is a theory and not a fully defined, documented, and verified idea, professionals have differing opinions about what mental processes are involved.
Normal ‘executive functioning’ may involve abilities such as:
- Estimating and visualizing outcomes
- Analyzing sights, sounds, and physical sensory information
- Perceiving and estimating time, distance, and force
- Anticipating consequences
- Mentally evaluating possible outcomes of different problem-solving strategies
- Acting, based on the likelihood of positive outcomes
- Choosing the most appropriate action based on social expectations and norms
- Performing tasks necessary to carry out decisions
< My Thoughts > “…without mindful awareness.”
While our brain’s executive functioning goes on throughout life without mindful awareness, it seems to become less visible during the ‘teenage’ years. The ‘teen brain’ is one of wonder.
NIH Staff Writer (2020) – Seven things to know about the ‘teen brain’ –
1. The brain reaches its biggest size in early adolescence. For girls this happens at 11 years of age; for boys its 14 years of age.
2. The brain continues to mature after it has stopped growing. The prefrontal cortex is one of the last regions to mature. This is responsible for skills like planning, prioritizing, and controlling impulses.
3. The teen brain is ready to learn and adapt. It has lots of plasticity, likes creative activities and changes and learns according to experiences and the environment.
4. Many mental disorders may begin to appear during adolescence. The mental disorders which can emerge during this period are – schizophrenia, anxiety disorder, depression, bipolar, and eating disorders.
5. Teen brains may be more vulnerable to stress as they respond differently than adults. Learning ‘meditation and mindfulness’ might help teens cope to reduce stress.
6. Teens need more sleep than children or adults. The sleep hormone levels of Melatonin shift and may cause teens to stay up late and struggle with getting up in the morning.
7. The teen brain is resilient, although vulnerable during this phase of development. Usually, teens get through this period to go on to become healthy adults.
< My Thoughts > “…phase of development.”
What happens when ‘cognition’, the mental process requiring knowledge & understanding of what one is experiencing in their environment, and the ‘phase of development’ of the teenage brain, and the lifelong cognition issues of an individual with autism COLLIDE? Added to this, the ordinary physical and emotional problems one experiences during adolescence can become overwhelming for any parent to deal with.
Ballan & Freyer (2017) found that some may consider the adolescent with ASD as a perpetual child, failing to acknowledge emerging sexual needs and issues. While a child’s public display of affection may seem appropriate for his/her developmental age, it could be disturbing, due to a mature physical appearance. Often ‘sexual education’ is provided only after the person demonstrated problematic sexual behavior. They found that with the help of Mental Health professionals, persons with autism could learn to cope with the physical, social, and emotional transitions of puberty, before the chance of issues arising. Some of the therapies discussed in the study were Cognitive Behavioral Therapy (CBT), Applied Behavior Analysis (ABA), and the use of Social Stories.
Note: More about Cognitive-Behavioral Therapy (CBT); more about Sexual Behavior in UNIT 4, Ch. 2; & Applied Behavior Analysis (ABA) in UNIT 7-2 on Complementary and Alternative Medicine (CAMs)
< My Thoughts > “…learn to cope…”
The degree to which an autistic child, adolescent, and/or adult will respond to helpful therapy depends upon the developmental levels and the cognitive abilities of the person with autism. And, most therapy can only provide ways to lessen symptoms, or to learn how to cope with sensory needs; as the ‘core’ symptoms of autism seem to be lifelong.
Davide-Rivera (2013) discusses how unchanging routines played a part in her life. For instance, a Fall scene played itself over and over again. The leaves dried up, snow fell, flowers bloomed, and days changed, but the routine never changed.
I don’t like interruption. If I am interrupted it is impossible to resume what I was doing without delay. My brain needs time to make the switch.
When I am writing, and the phone rings, or the kids interrupt, it takes a few minutes to even process what is going on. Mostly I am angered by the interruption, even today as an adult.
Freeman & Muraven (2010) tell us that ‘task interruption’ is especially harmful to a person with limited self-resources, and particularly so if they are close to the completion of that task, or it is a task that they are enjoying.
The interruption can be just a trivial irritation, if the person didn’t like the task, to becoming angry and impulsive. This has to do with self-control and self-regulation which could bring on frustration with stopping and starting an activity. The more often it occurs, the more negative the person’s response is to being interrupted.
Jones (2013) candidly admits, I often find myself unable to do something I could easily do the day before.
< My Thoughts > “…something I could do the day before.”
Parents and teachers are often completely puzzled by this kind of event. We make all kinds of excuses… ‘having a bad day’. ‘Must have forgotten from one day to the next’. ‘Not feeling cooperative today’. And, so on. No, you don’t have the correct answer. Oh sure, sometimes there could be any or all of those reasons, but probably it’s because the neuro-passages are not connecting at that moment in time.
Teachers may even get a note from the parent – “She seems to have forgotten how to pull up her pants. Are you still working on that at school? We have to be consistent with her you know.” And, I’m certain the parents have had a note with the reverse message from school. “Are you still working on that at home? We have to be consistent with her you know.”
Some days our brains are firing on all cylinders and some days they simply are not. You have probably experienced this yourself. We ‘neuro-typicals’ just go get a latte and move on. People with autism can’t seem to make just drinking a latte work for them.
Sohn (2020) says that even today, doctors often conflate autism and intellectual disability. That the biological distinction between them can be murky. And, that scientific progress depends on knowing where the conditions intersect – and part ways. In the clinic, though, clearer diagnosis would lead people to services more appropriate for them. On the other hand, they also know what kinds of doors open to those with an autism diagnosis, so they may err on the side of autism if they are not sure.
< My Thoughts > “…err on the side of autism…”
This could lead to a misdiagnosis sending children on another intervention trajectory altogether. Disappointing, when early and correct diagnoses are so important, to say nothing of the private and insurance monies which may be spent in error.
Nordahl (2018) talks on YouTube about a research study looking at 112 boys and 27 girls with autism between age three and five years, as well as a control sample of 53 boys and 29 girls without autism. Using a process called diffusion tensor imaging, the researchers looked at the corpus callosum—the largest neural fiber bundle in the brain—in the young kids. Prior research has shown differences in that area of the brain among people with autism. They found that the organization of these fibers was different in boys compared to girls, especially in the frontal lobes which play a role in executive functions.
Buxhoeveden, et al. (2006) believe that the frontal lobe is involved with the kind of higher-order cognitive, language and socio-emotional functions that are impaired in autism. The scarcity of developmental anatomical evidence requires the necessity of MRI studies in young children, 2 – 4 years old. With further of these studies, they are finding that failure of the cortical area to grow has resulted in narrow vertical ‘microorganization’; thus, reducing the child’s ability to generalize. This brain feature, it is suggested, enhances specialization abilities. The failure of the frontal cortex to continue growing suggests the normal process of brain growth has been stunted.
< My Thoughts > “…enhances specialization and reduces generalization…”
‘Enhanced specialization’ and ‘reduced generalization’ becomes concerning to most parents. Their rigid behavior becomes annoying and worrisome. Let’s say that their child becomes focused/specialized in one area. That area may be the distinct shape, feature, and color of a certain dinosaur. Or, the features of car license plates. Perhaps they spend the whole day lining up cars by size, model, or color. But when that same child is asked to’ generalize’ a similar action in a ‘sorting’ activity, they have no idea how to do it.
According to Bogdashina & Casanova (2016), deficits in planning, organizing and monitoring progress towards a goal often prevents one from taking a flexible approach to problem-solving. “Poor Executive Function can easily account for the lack of thinking flexibility and explains the rigidity of thinking exhibited by autistic people, including starting and finishing tasks which include all of the above.”
< My Thoughts > “…which include all of the above.”
One of the reasons that an autism diagnosis may come during the beginning school years could be due to ‘all of the above’. When the classroom demands which are made on a child extend beyond his or her executive functioning capabilities, then the ‘red flags’ go up, causing parents and teachers to become concerned.
Davide-Rivera (2013) – As a child, I was carefree – happy, as I knew happy to be at the time. But when I grew into a young woman life got messy, and continued to come unraveled as time went on. I had difficulty making friends, raising children, and communicating with my husband largely due to my autism.
It took 38 years for me to be diagnosed with Asperger’s Syndrome (AS), as a form of high functioning autism – 38 years of confusing experiences.
One of the first things that I learned about my Asperger’s diagnosis is that there are three core ‘cognition’ deficits which accompany this condition – the lack of theory of mind, executive dysfunction, and weak central coherence.
Mandy (2013) makes it known that diagnostic tests often miss girls, especially if they are of average intelligence. And, if females are diagnosed, it is much later than their male equivalents. One reason is that repetitive behaviors present in more socially normative ways, as the symptoms of personality or anxiety disorders. He also explains that the current diagnostic assessments are based on the extensive study of ‘boys’ with autism.
< My Thoughts > “…tests often miss girls…”
When my special education classroom consisted mainly of middle-school boys, a student came to me from out of state, in the middle of the semester. She didn’t have an Individualized Education Program (IEP) and was placed with me until more data about an appropriate placement could be obtained. The experienced social worker assigned to our school suspected that this student had learning disabilities, had missed a lot of school, and/or could have an emotional disorder. Eventually, against the parent’s hopes, we convinced them that she required testing before we could place her into the mainstream general education classes. By the end of that school year, she was diagnosed as having Asperger’s Syndrome (AS), with possible passive-aggressive behavior/personality disorder. And, because her family moved around a lot, she had missed critical parts of her early foundational education.
Nordahl (2018) knows that the few studies of girls with autism which have been done have shown that girls can even be affected more severely than boys. They recommended that more girls be found and recruited for studies, intervention, and treatment.
REFERENCES: UNIT 3; CHAPTER 3 – COGNITION
Ballan, M. & Freyer, M. (2017). Autism Spectrum Disorder, Adolescence, & Sexuality Education: Suggested Interventions for Mental Health Professionals; Sexual & Disability Journal; V35, p261-273.
Bogdashina, O., & Casanova, M. (2016). Sensory Perceptual Issues in Autism & Asperger Syndrome; 2nd Edition, eBook.
Buxhoeveden, D., Semendeferi, J., et al. (2006). Reduced minicolumns in the Frontal Cortex of Patients with Autism; Neuropathology & Applied Neurobiology; V32, p483-491.
Cariello, C. (2015). What Color is Monday? How Autism Changed One Family for the Better; eBook Edition.
Case-Lo, C. (2014). What’s the Connection Between Autism & Inflammation?; Retrieved online from –
healthline.com/health-news/connection-between-inflammation-and-autism/
Cherry, K. (2020). What Is Cognition?; Retrieved online from – https://www.verywellmind.com/what-is-cognition-2794982/
Chess, S. & Thomas, A. (1995). Keep Your Child's Temperament In Mind When Analyzing Problems & Solutions; Brown University Child & Adolescent Behavior Letter; V11:6.
Cohen, K. (2011). Seeing Ezra: A Mother’s Story of Autism, Unconditional Love, and the Meaning of Normal; eBook 2011 Edition.
Davide-Rivera, J. (2013). Twirling Naked in the Streets and No One Noticed: Growing Up with Autism; eBook Edition.
Freeman, N., & Muraven, M. (2010). Don’t interrupt me! Task interruption depletes one’s limited resources; Motivation & Emotion V34:3, p. 230-241.
Hunter, W. (2015). How Children Learn to See Someone Else’s Perspective; Retrieved online from –https:/parentingforsocialchange.com/perspective-taking-html/
Jones, S. (2013). No You Don’t – Essays from an Unstrange Mind; eBook Edition.
Kuzma, J. (2012). Perspective-taking Skills; World Press. Also reprinted in https://www.speechand languagekids.com/
Mandy, W. (2013). DSM-5 May Better Serve Girls with Autism; Spectrum Opinion Viewpoint; May Issue.
NIH Staff Writer (2020). The Teen Brain: 7 Things to Know; U.S. National Institutes of Health; Retrieved online from – https://www.nimh.nih.gov/health/publications/
Nordahl, C. (2018). Brains Wired Differently; YouTube, Autism Research; Retrieved online from – https://neuroscience.ucdavis.edu/people/christine-nordahl/
Sohn, E. (2020). The Blurred Line Between Autism & Intellectual Disability; Autism Research News. Retrieved online from – https://www.spectrumnews.org/author/emilysohn
Staff Writer (2019). Temperament, the Preventative Ounce; Retrieved online from – preventativeoz.org/
TEMPERAMENT / PERSONALITY –

|

|

|
Brock, et al. (2012) associate temperament with ‘sensory’ features in children with Autism. They say that individual differences in ‘sensory processing’ may form the basis for aspects of a person’s temperament and personality.
The Three Sensory Constructs they speak of are 1. hyper-responsiveness, 2. hypo-responsiveness, and 3. seeking behavior; within the Nine Dimensions of Temperament.
Nine Dimensions of Temperament –
Temperament refers to the ‘how’ (dimension) of the behavior, rather than the ‘what’ (ability), and/or the ‘why’ (motivation). Temperament (the ‘how’) is seldom observable in an autistic child’s behavioral style. But ‘Temperament Profiles’ of autistic children do seem to differ from that of a typically developing child. Some researchers suggest that the individual temperament differences are due to the person’s ‘sensory processing’ issues. While others do NOT believe there is a relationship between temperament and personality within the three ‘sensory’ constructs of – hyper-responsiveness, hypo-responsiveness, and seeking behavior.
< My Thoughts > “…while others do not believe …”
Overlapping theories of a ‘relationship’ between ‘temperament’ and what could be due to the child’s three ‘sensory processing’ classifications. Sensory degrees, such as – ‘hyper’ or ‘hypo’ or ‘seeking’ processing, could each possibly be occurring or reoccurring during the same incident. Or, that person could possibly have ‘sensory integration’ issues which causes difficulty in determining what is happening around them. The distinction between a ‘temperament’ and/or a ‘sensory issue’ connection should be made by an experienced and qualified therapist.
They also say some researchers suggest that individual differences in ‘sensory’ processing may form the very basis for the aspects of ‘temperament’ and ‘personality’. That ‘over’-responsiveness in some aspects, while ‘under’-responsiveness in others could be the possible basis.
Fleishmann & Fleishmann (2012) ask – Was it possible there was more to our daughter Carly’s personality than we had thought? After all, Carly ‘was’ autism. ‘Autism’ in her tantrums, and ‘autism’ in her neediness. When you raise a severely disabled child, you begin to see the flaws above all else. There were momentary smiles; infrequent heartwarming acts of love, such as a snuggle and a giggle. Also though, there was a wall that couldn’t be breached, locking her in and us out. But bit by bit now, a few stones in the wall were beginning to crumble. Bit by bit we were rewarded with glimpses of Carly’s hidden personality. She was becoming like one of those cakes with the surprise charms and coins baked inside.
Thompson (2012) tells us that – to a child with autism, the world is a very confusing and sometimes a scary place. They don’t understand what people say to them nor, the meaning behind people’s actions. They don’t understand what will occur, in which order it will occur, or when it will occur. Children who don’t understand these things start building up a fear of ‘changes’. If a daily routine is changed, aggression occurs, directed to making their parents restore things to the way they ‘ought’ to be, before the ‘change’ – from the child’s perspective.
Thompson tells us that parents ask, “Is she ever going to be like other kids?” Or say, “Her rituals are driving us crazy!” “She has to be the first one in the car.” “If she isn’t, she starts kicking her mother or me, screaming, and throwing herself on the ground.” “She has to have things her way.” “She’s spoiled!”
Studies show that the child is NOT ‘spoiled’, the child has autism. She has no idea what awful thing is going to happen ‘if’ she doesn’t get in the car first. Changing routine for this child is possible, but it must be done in stages, over several days, or even weeks. No, you can’t just spring ‘change’ on her, that will send her into a panic.
< My Thoughts > “…send her into a panic.”
Some parents are ‘spontaneous’ by nature. They are instant ‘problem solvers’, changing-up things in the blink of an eye as necessity requires. But, this changing-up things in the blink of an eye can send a child with autism spinning out of control. Some children need to have a ‘social story’ about a ‘change’ which might occur. Knowing this can help family situations go more smoothly, with less drama. The caveat to this of course, in the event of ‘unsafe’ behavior ‘safety’ comes first! You must jump into action when your child is hurting self or others. Afterward, explaining the need for ‘change’ with a ‘social story’ or other type of clarification. But extreme vigilance is always in place when with someone with autism.
Hopefully, over time, you are learning something about your child’s temperament. Maybe you have found out that s/he is just a ‘rascal’ at heart. Or, like Sonny, has the sweetest of dispositions. So, how do you ‘know’ which is your child’s personality or temperament, and which response is the ‘core’ nature of your child’s autism? By learning about your child’s ‘responses’, you can begin to help your child. Beginning to understand the interventions which may work and those which probably won’t, at least not right now.
Note: See Social Stories in #3C, INDEX / APPENDICES.
The Three Sensory Constructs they speak of are 1. hyper-responsiveness, 2. hypo-responsiveness, and 3. seeking behavior; within the Nine Dimensions of Temperament.
Nine Dimensions of Temperament –
- Activity – level, tempo & frequency of motor functioning
- Rhythmicity – degree of regularity & repetitive functioning
- Distractibility – interference of environment on behavior
- Approach –initial reaction to new stimulus or procedures
- Adaptability – ease or difficulty of response to behavior modification
- Persistence – determination to maintain or continue in face of intervention
- Threshold – extrinsic stimulation necessary to evoke a discernible response
- Intensity – energy content of response, irrespective of the negative / positive nature
- Mood – amount of pleasant, joyful, friendly behavior as contrasted by the opposite
Temperament refers to the ‘how’ (dimension) of the behavior, rather than the ‘what’ (ability), and/or the ‘why’ (motivation). Temperament (the ‘how’) is seldom observable in an autistic child’s behavioral style. But ‘Temperament Profiles’ of autistic children do seem to differ from that of a typically developing child. Some researchers suggest that the individual temperament differences are due to the person’s ‘sensory processing’ issues. While others do NOT believe there is a relationship between temperament and personality within the three ‘sensory’ constructs of – hyper-responsiveness, hypo-responsiveness, and seeking behavior.
< My Thoughts > “…while others do not believe …”
Overlapping theories of a ‘relationship’ between ‘temperament’ and what could be due to the child’s three ‘sensory processing’ classifications. Sensory degrees, such as – ‘hyper’ or ‘hypo’ or ‘seeking’ processing, could each possibly be occurring or reoccurring during the same incident. Or, that person could possibly have ‘sensory integration’ issues which causes difficulty in determining what is happening around them. The distinction between a ‘temperament’ and/or a ‘sensory issue’ connection should be made by an experienced and qualified therapist.
They also say some researchers suggest that individual differences in ‘sensory’ processing may form the very basis for the aspects of ‘temperament’ and ‘personality’. That ‘over’-responsiveness in some aspects, while ‘under’-responsiveness in others could be the possible basis.
Fleishmann & Fleishmann (2012) ask – Was it possible there was more to our daughter Carly’s personality than we had thought? After all, Carly ‘was’ autism. ‘Autism’ in her tantrums, and ‘autism’ in her neediness. When you raise a severely disabled child, you begin to see the flaws above all else. There were momentary smiles; infrequent heartwarming acts of love, such as a snuggle and a giggle. Also though, there was a wall that couldn’t be breached, locking her in and us out. But bit by bit now, a few stones in the wall were beginning to crumble. Bit by bit we were rewarded with glimpses of Carly’s hidden personality. She was becoming like one of those cakes with the surprise charms and coins baked inside.
Thompson (2012) tells us that – to a child with autism, the world is a very confusing and sometimes a scary place. They don’t understand what people say to them nor, the meaning behind people’s actions. They don’t understand what will occur, in which order it will occur, or when it will occur. Children who don’t understand these things start building up a fear of ‘changes’. If a daily routine is changed, aggression occurs, directed to making their parents restore things to the way they ‘ought’ to be, before the ‘change’ – from the child’s perspective.
Thompson tells us that parents ask, “Is she ever going to be like other kids?” Or say, “Her rituals are driving us crazy!” “She has to be the first one in the car.” “If she isn’t, she starts kicking her mother or me, screaming, and throwing herself on the ground.” “She has to have things her way.” “She’s spoiled!”
Studies show that the child is NOT ‘spoiled’, the child has autism. She has no idea what awful thing is going to happen ‘if’ she doesn’t get in the car first. Changing routine for this child is possible, but it must be done in stages, over several days, or even weeks. No, you can’t just spring ‘change’ on her, that will send her into a panic.
< My Thoughts > “…send her into a panic.”
Some parents are ‘spontaneous’ by nature. They are instant ‘problem solvers’, changing-up things in the blink of an eye as necessity requires. But, this changing-up things in the blink of an eye can send a child with autism spinning out of control. Some children need to have a ‘social story’ about a ‘change’ which might occur. Knowing this can help family situations go more smoothly, with less drama. The caveat to this of course, in the event of ‘unsafe’ behavior ‘safety’ comes first! You must jump into action when your child is hurting self or others. Afterward, explaining the need for ‘change’ with a ‘social story’ or other type of clarification. But extreme vigilance is always in place when with someone with autism.
Hopefully, over time, you are learning something about your child’s temperament. Maybe you have found out that s/he is just a ‘rascal’ at heart. Or, like Sonny, has the sweetest of dispositions. So, how do you ‘know’ which is your child’s personality or temperament, and which response is the ‘core’ nature of your child’s autism? By learning about your child’s ‘responses’, you can begin to help your child. Beginning to understand the interventions which may work and those which probably won’t, at least not right now.
Note: See Social Stories in #3C, INDEX / APPENDICES.
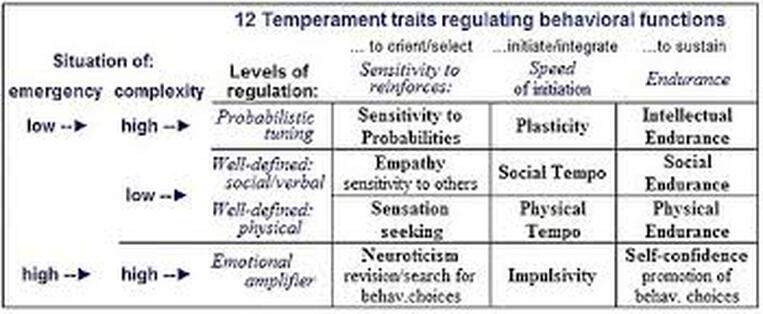
Temperament Scale
Temperament develops over one’s life span, reinforced by one’s experiences. One temperament scale shows a person can be seen by others as being –
So how does a parent decide which describes their child? Well, there are several assessments out there; mainly it’s a matter of relying on observations and parental intuition about the things which are occurring.
Lord (2012), (Sister) laments – One of my old Barbie dolls sits on the gravel, her arm raised in a friendly wave. David’s RULE: No toys in the fish tank. I write down all David’s rules, so my ‘someday-he’ll-wake-up-brother’ will know how the world works.
(Brother) “It’s five o’clock. Let’s go to the video store!”
(Sister) My hands squeeze into fists. Sometimes I wish someone would invent a pill so David’s wake up one morning without autism. But there is no pill.
Green (2013) tells us that smaller families seem to have more difficulty when dealing with the autistic child. That a sibling may have difficulties with feeling the loss of the normal sibling that ‘could have been’ if they didn’t have autism.
Lord (2012) (Brother) “It’s Mom!” “Let’s go to the video store!”
(Sister) “You’re going to occupational therapy.”
(Brother, frowning) “Let’s go to the video store.”
(Sister) “You’re going to OT,” I cover David’s mouth so people won’t hear him scream. I am twelve now and can stay home if I want, but I still like to come because I get Mom completely to myself.
< My Thoughts > “…I get Mom completely to myself.”
While her brother is in with the therapist, ‘sister’ has mom completely to herself. There are times as an educator, as well as a parent, when dealing with an autistic child’s severe behavior can become all consuming, requiring hyper-vigilance. Sometimes even requiring tuning-out everything and everyone else, in order to focus on the situation at-hand. Often, in the special education classroom setting, when the teacher engages one-on-one with a student in crisis, the domino effect occurs. One child in crisis ‘sets off’ other children who are on the verge of a meltdown themselves. Please, for the safety of all, never question why there should be at least two trained professionals in a special education classroom, at all times.
Rivers & Stoneman (2008) say that it is important to know what the typically developing siblings in their study had to say. Siblings expressed their overall ‘happiness’ at being included in helping their parents understand their ‘need’ to feel included. Also, they wanted to be part of predicting and dealing with the ASD sibling’s challenging behavior. “When my parents include me, I feel like an ‘insider’, not an ‘outsider’ to what is going on with my parent’s attention.”
< My Thoughts > “…I feel like an ‘insider’, not an ‘outsider’… “
Both the siblings and the non-involved parent may feel like ‘outsiders’ when not included in the timing, or the importance of the many interventions which they themselves must adjust their lives around.
Tsao, et al. (2012), remind us that while parenting in families of children with disabilities may include ‘favoring’ that disabled child, parents learn that their ‘parenting style’ also changes over time. However, the siblings’ perceptions of that parent’s favoritism may persist. And as a result, siblings often experience extreme loneliness.
Siri & Lyon (2014) say that mastering the functional capacities of the ‘whole child’ will help that child move up the ‘developmental ladder’. Strengthening the ‘whole child’ means attending to regulating their nervous system, their broad range of emotions, and their all-encompassing environment. It means helping them to communicate physically and verbally. This will be a beginning, a way to lead them towards independence.
< My Thoughts > “…the ‘whole child’…”
In my explorations through the literature, I’ve read that it may be difficult to discern between what are strong personality traits when they are mixed in with core autism traits. So, I’m wondering if we could ‘assume’ that your child – without autism – would be naturally outgoing and charming. Would s/he be likely to have strong eye contact when interacting with others? ‘Thespian’ traits, so to speak. This ‘may’, just ‘may’ explain why some children with ASD will naturally make eye contact and be charming. Explaining why some parents and educators reject the idea of autism, in the beginning. This could hold true of other traits which could be ‘hard wired’ through the gene pool, but are atypical when it comes to autism.
Cariello (2015) reflects about her son – At times you are going to marvel at his progress, his giant leaps in communication and social behavior. Then for a while, nothing. His development will level off, and you’ll fight a rising panic that he’ll never move forward again. Don’t worry. Like the steps on a staircase, his personality and behavior patterns will jump up and then stand still for a while. He’s eight now, and I can’t wait for you to meet him.
< My Thoughts > “…his personality and behavior patterns will jump…”
Some say persons are both ‘hard-wired’, meaning ‘born with’ certain behavior tendencies. Or, ‘soft-wired’, meaning that it’s ‘experiential learning’ which influences most behavior. Both types of wiring seemed to be designed for ‘survival’ and for responding to one’s environment. This may be the reason we see those personality and behavior changes over time.
Tancredi (2010) writes that our freedom, or free-will, may be limited because the ‘biological forces’ produced by the genes and by the environment, may be more powerful than anyone believes. Or, that the prefrontal cortex, which acts as the ‘command post’, may be the ‘ruler’ of our actions, after all.
Rivers & Stoneman (2008), in a study of 50 families found that ‘temperament’ is a relatively stable individual difference or characteristic. Saying that ‘temperament’ is rooted in the child’s biology, and influenced as the child develops by the environment and their maturity. For example, the child with undesirable Impulsivity is having a problem with their negative emotions and self-control. Or, the child who prefers ‘giving up’ versus ‘conscientiousness’ may always be refusing to complete a task, versus staying with it, even if the child perceives the task or problem as too difficult. Knowing this helps with the wisdom of ‘differential parenting.’
< My Thoughts > “…‘differential parenting.’
In understanding ‘differential parenting’, one would expect that siblings may feel that they are parented differently, while each is being raised in the same environment. For instance, some parents, albeit unknowingly, can be more open and empathetic to one child, as opposed to another. Or, the opposite parental attitude can be at work. In cases of families having a child with autism, one parent may silently be thought to favor or resent that child, in the eyes of the other children; or even in the eyes of the other parent. In other words – parent’s temperament meets child’s temperament.
The study also revealed ‘how’ brothers and sisters observed and interacted with their ASD sibling. They characterized their ASD sibling by saying that s/he had lower activity levels, lower emotional intensity, and was becoming more temperamentally difficult with time. The authors noted too that there seemed to be a gender distinction in the siblings, between how the girls (slightly more empathetic approach) seemingly responded to the situation, compared to the boys (slightly less empathetic approach).
Siblings noted that when parents acted ‘differently’ towards each of their typically developing children, they usually understood. Also, for the most part, they understood the ‘parental difference’ towards their ASD sibling’s behavior; not trying ‘regressing’ behavior, in order to get their parents’ attention.
< My Thoughts > “…‘parental difference’…”
Often, one may make a more acceptable ‘parental difference’ by assuming the role of ‘coach’ with your neuro-typical children. Possibly, that is a way in which you can more readily match that child’s needs, preferences, and strengths. In other words, perhaps acting more as you would as a ‘coach’ on a sports team. Give each child more of a positive ‘team’ success experience by motivating and renewing their spirit. By praising the good things and redirecting or guiding the undesirable behaviors, there may be a more productive, more positive result.
Brodie (2014) brings back memories of his brother, Scott. One time he seemed agitated and wanted something from the fridge. I walked by and saw so I stopped to open it for him. I was having difficulty with the combination lock. Suddenly, he pushed me towards the fridge, really hard. I think that was the moment I realized Scott had the temper of a toddler, but the strength of a man.
Green (2013) says “Siblings eventually develop awareness that the individual with ASD is often unable to control their behavior, resulting in some forbearance on the part of the sibling.” This may result in the sibling feeling unsafe and anxious when left alone with their autistic brother or sister.
Brodie (2014) continues, saying ‘Secondhand’ autism is not terminal. Autism does not typically include any shortened life expectancy, nor does secondhand autism. But autism is for life. Secondhand autism is less about the physical effects on the family members than the emotional and personality effects.
< My Thoughts > “emotional and personality effects.”
While parents, and sometimes older siblings are shuttling the child with autism back and forth to various schools, therapies, and/or interventions, consider that ‘other’ family members may also be in need of help.
Barry & Singer (2001) found many families were in crisis because of the autistic child’s aggressive behaviors towards the newest infant family member. These families solved the problem by finding a program designed for retraining the child with autism with appropriate replacement skills. “The child learned to interact with his new infant sibling in new ways. As the child’s aggressive behavior was reduced, the parents allowed him more access to the infant. And, as the sibling relationship develops, there are ‘continued interventions’ provided and more complicated skills will be taught.”
Sicile-Kira (2014), agrees that “No matter how bad the situation, there is always a solution. And mainly it is the parent’s attitude that will make the difference.”
More about TEMPERAMENT –
Temperament develops over one’s life span, reinforced by one’s experiences. One temperament scale shows a person can be seen by others as being –
- Cooperative
- Excitable
- Risk taker
- Defiant confrontational
- Stressed
So how does a parent decide which describes their child? Well, there are several assessments out there; mainly it’s a matter of relying on observations and parental intuition about the things which are occurring.
Lord (2012), (Sister) laments – One of my old Barbie dolls sits on the gravel, her arm raised in a friendly wave. David’s RULE: No toys in the fish tank. I write down all David’s rules, so my ‘someday-he’ll-wake-up-brother’ will know how the world works.
(Brother) “It’s five o’clock. Let’s go to the video store!”
(Sister) My hands squeeze into fists. Sometimes I wish someone would invent a pill so David’s wake up one morning without autism. But there is no pill.
Green (2013) tells us that smaller families seem to have more difficulty when dealing with the autistic child. That a sibling may have difficulties with feeling the loss of the normal sibling that ‘could have been’ if they didn’t have autism.
Lord (2012) (Brother) “It’s Mom!” “Let’s go to the video store!”
(Sister) “You’re going to occupational therapy.”
(Brother, frowning) “Let’s go to the video store.”
(Sister) “You’re going to OT,” I cover David’s mouth so people won’t hear him scream. I am twelve now and can stay home if I want, but I still like to come because I get Mom completely to myself.
< My Thoughts > “…I get Mom completely to myself.”
While her brother is in with the therapist, ‘sister’ has mom completely to herself. There are times as an educator, as well as a parent, when dealing with an autistic child’s severe behavior can become all consuming, requiring hyper-vigilance. Sometimes even requiring tuning-out everything and everyone else, in order to focus on the situation at-hand. Often, in the special education classroom setting, when the teacher engages one-on-one with a student in crisis, the domino effect occurs. One child in crisis ‘sets off’ other children who are on the verge of a meltdown themselves. Please, for the safety of all, never question why there should be at least two trained professionals in a special education classroom, at all times.
Rivers & Stoneman (2008) say that it is important to know what the typically developing siblings in their study had to say. Siblings expressed their overall ‘happiness’ at being included in helping their parents understand their ‘need’ to feel included. Also, they wanted to be part of predicting and dealing with the ASD sibling’s challenging behavior. “When my parents include me, I feel like an ‘insider’, not an ‘outsider’ to what is going on with my parent’s attention.”
< My Thoughts > “…I feel like an ‘insider’, not an ‘outsider’… “
Both the siblings and the non-involved parent may feel like ‘outsiders’ when not included in the timing, or the importance of the many interventions which they themselves must adjust their lives around.
Tsao, et al. (2012), remind us that while parenting in families of children with disabilities may include ‘favoring’ that disabled child, parents learn that their ‘parenting style’ also changes over time. However, the siblings’ perceptions of that parent’s favoritism may persist. And as a result, siblings often experience extreme loneliness.
Siri & Lyon (2014) say that mastering the functional capacities of the ‘whole child’ will help that child move up the ‘developmental ladder’. Strengthening the ‘whole child’ means attending to regulating their nervous system, their broad range of emotions, and their all-encompassing environment. It means helping them to communicate physically and verbally. This will be a beginning, a way to lead them towards independence.
< My Thoughts > “…the ‘whole child’…”
In my explorations through the literature, I’ve read that it may be difficult to discern between what are strong personality traits when they are mixed in with core autism traits. So, I’m wondering if we could ‘assume’ that your child – without autism – would be naturally outgoing and charming. Would s/he be likely to have strong eye contact when interacting with others? ‘Thespian’ traits, so to speak. This ‘may’, just ‘may’ explain why some children with ASD will naturally make eye contact and be charming. Explaining why some parents and educators reject the idea of autism, in the beginning. This could hold true of other traits which could be ‘hard wired’ through the gene pool, but are atypical when it comes to autism.
Cariello (2015) reflects about her son – At times you are going to marvel at his progress, his giant leaps in communication and social behavior. Then for a while, nothing. His development will level off, and you’ll fight a rising panic that he’ll never move forward again. Don’t worry. Like the steps on a staircase, his personality and behavior patterns will jump up and then stand still for a while. He’s eight now, and I can’t wait for you to meet him.
< My Thoughts > “…his personality and behavior patterns will jump…”
Some say persons are both ‘hard-wired’, meaning ‘born with’ certain behavior tendencies. Or, ‘soft-wired’, meaning that it’s ‘experiential learning’ which influences most behavior. Both types of wiring seemed to be designed for ‘survival’ and for responding to one’s environment. This may be the reason we see those personality and behavior changes over time.
Tancredi (2010) writes that our freedom, or free-will, may be limited because the ‘biological forces’ produced by the genes and by the environment, may be more powerful than anyone believes. Or, that the prefrontal cortex, which acts as the ‘command post’, may be the ‘ruler’ of our actions, after all.
Rivers & Stoneman (2008), in a study of 50 families found that ‘temperament’ is a relatively stable individual difference or characteristic. Saying that ‘temperament’ is rooted in the child’s biology, and influenced as the child develops by the environment and their maturity. For example, the child with undesirable Impulsivity is having a problem with their negative emotions and self-control. Or, the child who prefers ‘giving up’ versus ‘conscientiousness’ may always be refusing to complete a task, versus staying with it, even if the child perceives the task or problem as too difficult. Knowing this helps with the wisdom of ‘differential parenting.’
< My Thoughts > “…‘differential parenting.’
In understanding ‘differential parenting’, one would expect that siblings may feel that they are parented differently, while each is being raised in the same environment. For instance, some parents, albeit unknowingly, can be more open and empathetic to one child, as opposed to another. Or, the opposite parental attitude can be at work. In cases of families having a child with autism, one parent may silently be thought to favor or resent that child, in the eyes of the other children; or even in the eyes of the other parent. In other words – parent’s temperament meets child’s temperament.
The study also revealed ‘how’ brothers and sisters observed and interacted with their ASD sibling. They characterized their ASD sibling by saying that s/he had lower activity levels, lower emotional intensity, and was becoming more temperamentally difficult with time. The authors noted too that there seemed to be a gender distinction in the siblings, between how the girls (slightly more empathetic approach) seemingly responded to the situation, compared to the boys (slightly less empathetic approach).
Siblings noted that when parents acted ‘differently’ towards each of their typically developing children, they usually understood. Also, for the most part, they understood the ‘parental difference’ towards their ASD sibling’s behavior; not trying ‘regressing’ behavior, in order to get their parents’ attention.
< My Thoughts > “…‘parental difference’…”
Often, one may make a more acceptable ‘parental difference’ by assuming the role of ‘coach’ with your neuro-typical children. Possibly, that is a way in which you can more readily match that child’s needs, preferences, and strengths. In other words, perhaps acting more as you would as a ‘coach’ on a sports team. Give each child more of a positive ‘team’ success experience by motivating and renewing their spirit. By praising the good things and redirecting or guiding the undesirable behaviors, there may be a more productive, more positive result.
Brodie (2014) brings back memories of his brother, Scott. One time he seemed agitated and wanted something from the fridge. I walked by and saw so I stopped to open it for him. I was having difficulty with the combination lock. Suddenly, he pushed me towards the fridge, really hard. I think that was the moment I realized Scott had the temper of a toddler, but the strength of a man.
Green (2013) says “Siblings eventually develop awareness that the individual with ASD is often unable to control their behavior, resulting in some forbearance on the part of the sibling.” This may result in the sibling feeling unsafe and anxious when left alone with their autistic brother or sister.
Brodie (2014) continues, saying ‘Secondhand’ autism is not terminal. Autism does not typically include any shortened life expectancy, nor does secondhand autism. But autism is for life. Secondhand autism is less about the physical effects on the family members than the emotional and personality effects.
< My Thoughts > “emotional and personality effects.”
While parents, and sometimes older siblings are shuttling the child with autism back and forth to various schools, therapies, and/or interventions, consider that ‘other’ family members may also be in need of help.
Barry & Singer (2001) found many families were in crisis because of the autistic child’s aggressive behaviors towards the newest infant family member. These families solved the problem by finding a program designed for retraining the child with autism with appropriate replacement skills. “The child learned to interact with his new infant sibling in new ways. As the child’s aggressive behavior was reduced, the parents allowed him more access to the infant. And, as the sibling relationship develops, there are ‘continued interventions’ provided and more complicated skills will be taught.”
Sicile-Kira (2014), agrees that “No matter how bad the situation, there is always a solution. And mainly it is the parent’s attitude that will make the difference.”
More about TEMPERAMENT –
< My Thoughts > The BIG FIVE model of personality assessment is one of several models that are out there in the world of psychology & psychiatry. Here is one just focused on children.
Temperament Assessment Scale for Children –
By answering the following questions, you may increase your understanding of the temperament of your child.
1. Activity Level. How much does the child wiggle & move around when being read to, sitting, or playing alone?
High Activity 1 3 5 Low Activity
2. Regularity. Is the child regular about eating times, sleeping times, & bowel movements?
Regular 1 3 5 Irregular
3. Adaptability. How quickly does the child adapt to changes in his/her schedule or routine? Or, adapt to new places?
Adapts quickly 1 3 5 Slow to adapt
4. Approach/Withdrawal. How does the child usually react the 1st time to new people, foods, toys, & activities?
Approaches 1 3 5 Withdraws
5. Physical Sensitivity. How aware is the child of small differences in noise, temperature, taste, & clothing?
Not sensitive 1 3 5 Very sensitive
6. Intensity of Reaction. How strong or violent are the child's reactions? Does the child laugh & cry energetically, or does s/he just smile & fuss mildly?
High intensity 1 3 5 Mild reaction
7. Distractibility. Is the child easily distracted, or does s/he ignore distractions? Will the child continue to work or play when others are present?
Very distractible 1 3 5 Not distractible
8. Positive or Negative Mood. How much of the time does the child show pleasant, joyful behavior compared with unpleasant crying & fussing behavior?
Positive mood 1 3 5 Negative mood
9. Persistence. How long does the child continue with one activity? Does the child usually get distracted if it’s perceived to be too difficult?
Long focus span 1 3 5 Short focus span
10. Emotional Sensitivity. How does your child respond emotionally to understanding feelings of self & others?
Not sensitive 1 3 5 Very sensitive
Retrieved online from – Temperament Assessment Scale for Children – collab4kids.org/wp-content/uploads/2015/07/Symposium2015Griffin1.pdf/
Cariello (2015) knows that autism unfolds differently in each individual; some demonstrate symptoms very early on while others grow and interact normally for a while and then seemingly morph into another person altogether.
< My Thoughts > “…morph into another person altogether.”
Some professionals believe that instead of ‘morphing’, or taking on a variety of new forms, their brain waves are really ‘untangling’. Such as, the child seems okay and meeting their developmental milestones, when suddenly they seem to ‘regress’.
Over the course of seven years, Cariello says, Jack had changed so much from that initial list of autism symptoms; he was a different boy entirely. He is now extremely affectionate and loving. For example, he can finish my sentences and read nonverbal cues, such as a warning look from across the room.
< My Thoughts > “…extremely affectionate and loving…”
One of the main reasons a middle school student of mine was ‘disqualified’ for services was because he was usually ‘friendly’ and ‘affectionate’, and had a lot of language and conversation. By the time they become more clever adolescents, they see being friendly and talkative as a way to ‘manipulate’ their surroundings.
Soderstrom, et al. (2002) tell us more about TEMPERAMENT and Asperger’s – Many high functioning adolescents with ASD on the Asperger’s side of the spectrum may begin to notice how they differ from their peers. They can have significant social, emotional, and behavioral ‘differences’ which influence how they process their world.
Some ‘differences’ include –
Also, possibly interpreting others benign behavior as having hostile intent, due to negative feelings about themselves. Or, misperceiving others actions, actions or purpose.
< My Thoughts > “…misperceiving others actions, actions or purpose.”
Adolescents and adults with Asperger’s, while all on the Autism Spectrum, have different temperaments, wants, and emotional needs. It is important that as things change, the support and intervention for those needs can shift with them. The Asperger’s adolescent should have every opportunity to prepare for college and/or job training as the student with an ‘autism’ diagnosis. In their Individualized Education Plan (IEP) they should have an Individual Transition Plan to address this. Also needed is support against social awkwardness and for making and keeping friends close. This is mentioned because if the Asperger’s adolescent had an early diagnosis, prior to DSM-5 (2013), then their IEP may not have included a ‘transition plan’. One of the things to verify, as a parent or as a teacher.
Note: More about Individualized Education Plan (IEP) and Individual Transition Plan in Unit 6.
Marks (2012) tells us that she ran into an old friend at the shopping center, who was also autistic. Everyone says, “Hello,” but not Becky and not me. She stares at space or something behind me. We are both nervous. I have to walk away and I do mean, ‘Have To’. I do not know how to tell her I have missed her. I think she knows that. I hope she does. “Wait, Becky. I am sorry to run away,” echoes in my head. How different for us. No hugs, no kisses. Just glances. Click clack. Click clack. Click clack.
< My Thoughts > “Wait, Becky. I am sorry to run away…”
As a teacher, I’ve heard students admit that they would enjoy having a friend. But they just don’t want to see them every single day! Also, they say, “Sometimes I have unwanted anger reactions to things that they do. And, sometimes I do things that people don’t understand or can’t forgive. They admit that they do feel lonely sometimes, but just feel too different from other people to try to be their ‘forever’ friend.
Sicile-Kira (2014) says that “Social relationships are important to all people, yet are difficult for many on the autism spectrum to develop naturally. Having social skills, knowing about expected yet often unstated rules of behavior, and social boundaries. There are different ways of teaching what is needed to be learned about relationships.” Some of the things she suggests are – Social Skills Training, Social Stories, Social Thinking, and hidden rules such as ‘assumed knowledge’, social hierarchies, and expected/unexpected situations.
< My Thoughts > “…‘assumed knowledge’…”
Social experiences can go wonderfully right, or terribly wrong, depending on what the person understands about the social expectations. For social success, it is important to know the ‘hidden rules’ of social behavior, recognize social cues and act on them appropriately.
Some ‘differences’ include –
- intense anxiety in response to change
- fear of specific objects or unpredictable events
- frustration and anger related to an inability to understand social conventions
- anxious tenseness
- modulation of their attention
- obsessive behaviors
- severe temper tantrums & meltdowns
- resent intrusions from the outside world
- low tolerance or hyper-frustration with interruption of routines
- unusual intense emotional & behavioral reactions
- difficulty in understanding the feelings of others
- one-sided conversations
- want peer relationships, but can’t sustain them
- idiosyncrasies others don’t understand
Also, possibly interpreting others benign behavior as having hostile intent, due to negative feelings about themselves. Or, misperceiving others actions, actions or purpose.
< My Thoughts > “…misperceiving others actions, actions or purpose.”
Adolescents and adults with Asperger’s, while all on the Autism Spectrum, have different temperaments, wants, and emotional needs. It is important that as things change, the support and intervention for those needs can shift with them. The Asperger’s adolescent should have every opportunity to prepare for college and/or job training as the student with an ‘autism’ diagnosis. In their Individualized Education Plan (IEP) they should have an Individual Transition Plan to address this. Also needed is support against social awkwardness and for making and keeping friends close. This is mentioned because if the Asperger’s adolescent had an early diagnosis, prior to DSM-5 (2013), then their IEP may not have included a ‘transition plan’. One of the things to verify, as a parent or as a teacher.
Note: More about Individualized Education Plan (IEP) and Individual Transition Plan in Unit 6.
Marks (2012) tells us that she ran into an old friend at the shopping center, who was also autistic. Everyone says, “Hello,” but not Becky and not me. She stares at space or something behind me. We are both nervous. I have to walk away and I do mean, ‘Have To’. I do not know how to tell her I have missed her. I think she knows that. I hope she does. “Wait, Becky. I am sorry to run away,” echoes in my head. How different for us. No hugs, no kisses. Just glances. Click clack. Click clack. Click clack.
< My Thoughts > “Wait, Becky. I am sorry to run away…”
As a teacher, I’ve heard students admit that they would enjoy having a friend. But they just don’t want to see them every single day! Also, they say, “Sometimes I have unwanted anger reactions to things that they do. And, sometimes I do things that people don’t understand or can’t forgive. They admit that they do feel lonely sometimes, but just feel too different from other people to try to be their ‘forever’ friend.
Sicile-Kira (2014) says that “Social relationships are important to all people, yet are difficult for many on the autism spectrum to develop naturally. Having social skills, knowing about expected yet often unstated rules of behavior, and social boundaries. There are different ways of teaching what is needed to be learned about relationships.” Some of the things she suggests are – Social Skills Training, Social Stories, Social Thinking, and hidden rules such as ‘assumed knowledge’, social hierarchies, and expected/unexpected situations.
< My Thoughts > “…‘assumed knowledge’…”
Social experiences can go wonderfully right, or terribly wrong, depending on what the person understands about the social expectations. For social success, it is important to know the ‘hidden rules’ of social behavior, recognize social cues and act on them appropriately.
Cademy (2013) gives us Liz’s List of Female Asperger’s Syndrome (AS) Traits:
Appearance / Personal Habits –
- Eccentric personality; may be reflected in appearance.
- May not have a strong sense of identity and can be very chameleon-like, especially before diagnosis.
- May have been diagnosed as autistic or Asperger’s when young, or may have been thought of as gifted, shy, sensitive, etc. May also have had obvious or severe learning deficits.
- Often musical, artistic. May have a savant skill or strong talent.
- May have a strong interest in computers, games, science graphic design, inventing, things of a technological and visual nature. More AS verbal thinkers may gravitate to writing, languages, cultural studies, psychology.
- Can be very passionate about a course of study or job, and then change direction or go completely cold on it very quickly.
Greene (2014) offers, “Your child, at times, may appear as though s/he is actually capable of meeting a given expectation because s/he sometimes does. Often this leads the adult to believe that the child can meet that expectation when s/he feels like it.” “I know s/he can do it, s/he did it yesterday!!!
< My Thoughts > “…s/he did it yesterday!!!”
Just this fact alone can make parents and teachers a little bit ‘crazy’ when trying to explain or justify anything behavior related that you know the child/student has mastered, but won’t repeat on command. My theory is this – if the child knows, that you know that they know, then why are we playing the ‘Show me what you know” game? Never underestimate the genuine intelligence of a person with autism, especially those on the Asperger’s side of the spectrum.
Mesibov (2004) makes known a study which identifies and helps some of the unique ‘problem learning’ characteristics of students across the autism spectrum. This study offers learning strategies which can work towards a student’s strengths and interests. Taking them alphabetically, the study mentioned difficulty learning to overcome problems with – distractibility, generalization, organization, and sequencing.
- Distractibility takes many forms. Identifying the sources through careful assessment is crucial. The person may be distracted by the task, itself; by auditory and visual aspects of the environment, or, by things in the work area. A comfortable, well-designed space can help with this.
< My Thoughts > “…things in the work area.”
The woodgrain on a desk or table can mesmerize Sonny for hours, as he shuts out everything else around him.
- Generalization skills can often be taught by taking skills learned at home or at school into the community. Taking the person on a ‘field trip’, or introducing them to an interesting workplace may help.
< My Thoughts > “…into the community.”
During one Extended School Year (ESY Special Education summer school), I took a few of my students with another teacher and her students to a new fast-food café just off campus. We would be ‘generalizing’ skills such as – staying together in a group while walking from point A to point B; using all the ‘street crossing’ protocol; choosing and sitting at a lunch table; taking turns selecting, ordering, and paying for our food, etc. We then reversed the process, returning to campus and our classrooms. All went well, in fact better than expected.
Our ‘generalization’ outing was a big hit with everyone, including our principal. Until, the next day when my colleague came rushing into my room. “Have you seen Sally?” she asked. “I thought maybe she had come to your room.” We checked the bathrooms, the playground, and everywhere we thought she might go. Finally, we did an “All Call’ on the school intercom/loudspeaker. No Sally. Suddenly, I knew where she was. A call to the café’s manager confirmed that Sally was indeed there, sitting quietly at one of the tables.
- Organization is very complex learning characteristic, requiring planning, implementation, and the ability to overcome unforeseen obstacles. Helpful can be developing systematic habits and routines, established through visual schedules, checklists, and other visual instructions.
< My Thoughts > “…visual instructions.”
Having some type of age-appropriate visual instructions, as an ‘organizational’ guide, available for an independent look, can be very helpful, and will also encourage independence.
- Sequencing is difficult too, requiring tasks completed in correct order, working from right to left, and being able to see relationships. Learning and practicing these steps, until it becomes an established habit.
< My Thoughts > “…tasks completed in correct order…”
Some special education teachers say that ‘sequencing’ is the most difficult task to teach. One of the reasons may be because you begin with children at such an early age. Often, when young students start coming to the classroom, in pre-school or Kindergarten, they won’t leave their shoes and socks on. Probably because for the most part of the day at home they go shoeless. Teaching the sequence of ‘sitting down’, ‘putting on’ shoes and socks can be one of the first and most long lasting ‘sequencing’ challenges teachers and students face.
The Mesibov studies also show that learning to overcome problems with distractibility, generalization, organization, and sequencing must be addressed before the student can accomplish the most basic educational and workplace practices to a successful degree.
Johnson (2014) remembers, “I work as a Reading Interventionist and a Response to Intervention Coordinator in an elementary school. Every day, I work with students who struggle academically and/or socially. I have had experiences with children who have all sorts of disabilities; from learning disabilities, to intellectual disabilities, to autism. That wasn’t my daughter Sophie.”
< My Thoughts > “That wasn’t my daughter Sophie.”
Why didn’t she recognize the signs in her daughter Sophie? Because of the many different ways that autism presents, one may not recognize differences in their own child. Even a professional may think that it’s just the child’s temperament or personality. Then it may be that they tend to ignore the slow, regressive changes in behavior which indicates autism.
Senator (2006) stressed – To me, it was like a bad dream. Our sunny, silent, compliant little boy was changing into a stormy, loud, difficult child. “I don’t know what to do,” I said. “I’ve tried everything. You know I have.”
He doesn’t like other kids! Is that so terrible?” was my husband Ned’s reply.
We saw that Nat’s behaviors were the result of a combination of elements – his personality, growth factors (such as hormonal changes), and his autism. There is no way we could “fix” it all. No way to make him completely acceptable to the world. But, we decided, that what we can improve, we will, and medication offered opportunities for improvement.
What autism has taught us is that we can do many things to prepare Nat for adult life, to help him participate in the world, and yet it’s painfully clear that the world still is not ready for him. Nat’s brothers continue to buzz around him, interacting with him differently with each new phase of theirs. I still try to find a common denominator for all three.
REFERENCES: UNIT 3; CHAPTER 3 – TEMPERAMENT / PERSONALITY
Barry, L. & Singer, G. (2001). A Family in Crisis: Replacing the Aggressive Behavior of a Child with Autism Toward Infant Sibling; Journal of Positive Behavior Interventions; V3:1; p28-38.
Brock, M., Freuler, A. (2012). Temperament & Sensory Features of Children with Autism; Journal of Autism & Developmental Disorders; V42, p2271-2284.
Brodie, P. (2014). Secondhand Autism; eBook Edition.
Cademy, L. (2013). The Aspie Parent, the First Two Years A Collection of Posts from the Aspie Parent Blog; eBook Edition.
Cariello, C. (2015). What Color is Monday? How Autism Changed One Family for the Better; eBook Edition.
Fleishmann, A., & Fleishmann, C. (2012). Carly’s Voice: Breaking Through Autism; eBook Edition.
Green, L. (2013). The Well-Being of Siblings of Individuals with Autism; ISRN Neurology; V:2013; Art. 417194.
Greene, R. (2014). The Explosive Child; Harper Publishers, New York, N.Y.
Lord, C. (2012). Rules (for David); Scholastic Gold, Inc.
Marks, S. (2012). Paula’s Journal: Surviving Autism; eBook Edition.
Mesibov, G. (2004). Learning Styles of Students with Autism; Retrieved online from ASA, Univ. of N.C.; http://www.bridges4kids.org/
Johnson, I. (2014). The Journey to Normal: Our Family’s Life with Autism; eBook Edition.
Rivers, J., & Stoneman, Z. (2008). Child Temperaments, Differential Parenting, and the Sibling Relationships of Children with Autism Spectrum Disorder; Journal of Autism & Developmental Disorders; V38: p1740-1750.
Senator, S. (2006). Making Peace with Autism: One Family’s Story of Struggle, Discovery & Unexpected Gifts; eBook Edition.
Sicile-Kira, C. (2014). Autism Spectrum Disorder (revised): The Complete Guide to Understanding Autism; New York, New York: Penguin Random House Company.
Siri, K. & Lyons, T. (2014). Cutting-Edge Therapies for Autism; 4th Edition; Skyhorse Publishing, New York, N.Y.
Soderstrom, H., Rastam, M., et al. (2002). Temperament & Character in Adults with Asperger’s Syndrome; Retrieved online from – journals.sagepub.com/
Tancredi, L. (2010). Hardwired Behavior: What Neuroscience Teaches About Morality; Cambridge University Press; p226.
Thompson, T. (2012). Making Sense of Autism; Second Edition; Baltimore, Maryland: Brookes Publishing Company.
APPENDIX A – CHAPTER 3 Learning Disabilities:
Learning Disabilities: An Overview by: LD Online (2008); Retrieved online from – http://www.ldonline.org/article/5613/
In this article:
- What is a learning disability?
- What are the types of learning disabilities?
- Dyslexia (difficulty reading)
- Dysgraphia (difficulty writing)
- Dyscalculia (difficulty with mathematics)
- Other related conditions
What is a learning disability?
Some individuals, despite having an average or above average level of intelligence, have real difficulty acquiring basic academic skills. These skills include those needed for successful reading, writing, listening, speaking and/or math. These difficulties might be the result of a learning disability.
The Individuals with Disabilities Education Act (IDEA), a federal law, defines a learning disability as a condition when a child's achievement is substantially below what one might expect for that child. Learning disabilities do not include problems that are primarily the result of intellectual disabilities, emotional disturbance, or visual, hearing, emotional or intellectual disabilities. The official definition is here.
Many children with LD have struggled with reading. The difficulties often begin with individual sounds, or phonemes. Students may have problems with rhyming, and pulling words apart into their individual sounds (segmenting) and putting individual sounds together to form words (blending). This makes it difficult to decode words accurately, which can lead to trouble with fluency and comprehension. As students move through the grades, more and more of the information they need to learn is presented in written (through textbooks) or oral (through lecture) form. This exacerbates the difficulties they have succeeding in school.
What are the types of learning disabilities?
LD is a broad term. There are many different kinds of learning disabilities. Most often they fall into three broad categories:
- Reading disabilities (often referred to as dyslexia)
- Written language disabilities (often referred to as dysgraphia)
- Math disabilities (often called dyscalculia)
Other related categories include disabilities that affect memory, social skills, and executive functions such as deciding to begin a task.
Here is information on the more common forms of LD –
Dyslexia (difficulty reading)
Dyslexia is characterized by difficulties with accurate and/or fluent word recognition and by poor spelling and decoding abilities. Reading disabilities affect 2 to 8 percent of elementary school children. To read successfully, one must:
- Focus attention on the printed symbols
- Recognize the sounds associated with letters
- Understand words and grammar
- Build ideas and images
- Compare new ideas to what you already know
- Store ideas in memory
A person with dyslexia can have problems in any of the tasks involved in reading. However, scientists found that a significant number of people with dyslexia share an inability to distinguish or separate the sounds in spoken words. Some children have problems sounding out words, while others have trouble with rhyming games, such as rhyming "cat" with "bat." Yet, remedial reading specialists have found these skills fundamental to learning to read. Fortunately, specialists have developed techniques that can help many children with dyslexia acquire these skills. However, there is more to reading than recognizing words. If the brain is unable to form images or relate new ideas to those stored in memory, the reader cannot understand or remember the new concepts. Other types of reading disabilities can appear in the upper grades when the focus of reading shifts from word identification to comprehension.
< My Thoughts > “…rhyming "cat" with "bat."
A helpful way for a child to recognize the sounds associated with letters is to ask them how to change a ‘cat’ into a ‘bat’. The answer is simply change the first letter. Ask them what they would change the ‘bat’ into. Hopefully, they’ll say ‘rat’. This short activity delights and empowers resistant students. Also, providing Closed Captioning while watching TV.
Dysgraphia (difficulty writing)
Writing too, involves several brain areas and functions. The brain networks for vocabulary, grammar, hand movement, and memory must all be in good working order. A developmental writing disorder may result from problems in any of these areas. For example, a child with a writing disability, particularly an expressive language disorder, might be unable to compose complete and grammatically correct sentences.
Dyscalculia (difficulty with mathematics)
Arithmetic involves recognizing numbers and symbols, memorizing facts, aligning numbers, and understanding abstract concepts like place value and fractions. Any of these may be difficult for children with developmental arithmetic disorders, also called dyscalculia. Problems with number or basic concepts are likely to show up early. Disabilities that appear in the later grades are more often tied to problems in reasoning.
Note: More about Learning Disabilities in future chapters.
APPENDIX B – CHAPTER 3 – Theory of Mind (ToM)
Theory of Mind
Cariello, C. (2015) 57% Literal boys like Jack, will start looking around wildly for giraffes when their mother announces that the box store parking lot is a zoo!
21% As a literally thinker… he has trouble with cognitive flexibility and ‘theory of mind’. An aspect of social cognition, ‘theory of mind’ is the ability to understand that others have beliefs, opinions, and feelings different than your own. Jack however, thinks everyone sees and feels and likes the same things he does.
< My Thoughts > “…everyone sees and feels and likes the same things he does.”
Thinking that another’s life duplicates yours in every way, with the same wants and needs. Thinking they are experiencing the same feelings, perceptions, and environmental setting as you are experiencing.
Even neuro-typical’s with undeveloped or underdeveloped ‘Theory of Mind’ will believe that others think, understand, and perceive the world ‘exactly’ as they do. They do not realize that different persons have different thoughts, desires, beliefs, and attitudes by which they make sense of the world they live in.
Cariello, C. (2015) 23% How do you increase a person’s ‘theory of mind’ and help them understand that others think and feel differently?
With the help of our psychologist, we…created a strategy to increase his (Jack’s) ability in each of the identified areas:
- Self-regulation
- Communication
- Cognitive ability
< My Thoughts > “…skills he needed…”
Neurotypical persons naturally develop the needed ‘survival’ skills to interpret, predict, intuit, and imagine what others in their world are thinking. Persons with autism are mostly ‘literal’ thinkers like Jack. They are so focused on ‘their’ world that there is no room for anyone or anything else. While neurotypicals sometimes find it difficult to see and/or accept another’s point of view; persons with autism often find it impossible. Besides, what purpose would it serve them? They see no need, because they are so intensely certain that their way is the true one.
Staff Writer (2008) states, “In his 1995 book, Mind ness: An Essay on Autism and Theory of Mind," Simon Baron-Cohen explored what has become one of the central theoretical concepts of autism: theory of mind. Baron-Cohen proposed that children with autism suffer from ‘mindblindness’. Already hampered by the inability to achieve ‘joint attention’ with others, they become unable to build on that fundamental step to ‘intuit’ what others are thinking, perceiving, intending, or believing. They become “blind” to others’ mental states.
Staff Writer (2008) says that individuals with ASDs lack this ‘thinking ability’ to a staggering degree. They cannot read social cues; including facial expressions, body language, or tone of voice. Even higher functioning individuals who are trying to pay attention, who want to connect, constantly commit social mistakes, alienating their peers. They have a hard time noticing the social world and interpreting it.
Early problems with gaze and joint attention, it is believed, come to impact their ‘theory of mind’. ‘Theory of mind’ simply refers to the understanding that other people have their own thoughts, perceptions, and intentions separate from one’s own. It is part of seeing others as separate beings with their own agendas. To accommodate others, to predict their future behavior, to manipulate or please them, you must have this inbuilt capacity to guess something about who they are and what they might do or desire. Individuals with ASDs lack this ability to a staggering degree.
< My Thoughts > “…other people…”
Who are these ‘other’ people? “…’blind’ to others’ mental states… to a staggering degree…” Our Sonny only seems to need ‘others’ when he can’t get to something, needs you to fix his TV, or wants to go somewhere. He has no indication that you may have any priorities at all. You are there to ‘serve’ him. Much like an infant’s early life is self-focused, so that you exist only when needed.
We are tolerated only when it serves Sonny’s purpose. Thus, asking him to stock blocks, work a puzzle, or turn the pages in a book, often leaves him confused; because it serves him no purpose.
As a mother, I know this; but, as a teacher working with a student in the classroom, I sometimes forget that. As a Special Education teacher, I try to follow the curriculum, teach lessons, and engage special needs students in instruction. My students, however, are their primarily because they have been placed there against their will. Their day has been severely interrupted by delivering them to school. True, that on occasions, a ‘teachable moment’ occurs; fleeting as it may be. But basically, I am annoyingly intruding into their world, asking for behavior which serves no motivation to them.
Davide-Rivera, J. (2013) 92% It took 38 years for me to be diagnosed with Asperger’s Syndrome (AS), as a form of high functioning autism – 38 years of confusing experiences.
53% One of the first things that I learned about my Asperger’s diagnosis is that there are three core deficits that accompany this condition – the lack of theory of mind, executive dysfunction, and weak central coherence. There are also a host of other issues like sensory processing difficulties – being hyper or hypo sensitive to outside stimuli like to heat, cold, or pain.
< My Thoughts > “…the lack of theory of mind …”
Lack of ‘theory of mind (ToM),’ is also thinking that everyone is having the same ‘sensory experience’ that you are. Believing that everyone’s’ world mirrors yours exactly.
Cariello, C. & Capell, J. (2015) 11% I’ve often thought that Jack does not appear to experience a full range of emotions in the same way you or I might. His spectrum disorder seems to prohibit his emotional pendulum from swinging widely across a landscape of feelings that often include shame and humility and empathy and amusement. But after the initial shock of having broken his dad’s mug… the pendulum swung a little wider. He cycled a new set of emotions: sorrow, regret, and (to some degree) grief.
< My Thoughts > “…the pendulum swung a little wider.”
Children with autism may fail formal ‘theory of mind’ tests, but at times, show real-time understanding of another’s perspective. Especially, when the person with ASD is intimately involved. They get a glimpse of ‘cause & effect’. Momentarily, they may understand that the one thing that happened, has caused another thing to happen. Jack intuited that because he had broken his father’s favorite morning coffee mug, his dad couldn’t start his day. Interruption of ‘routine’ is devastating to those with ASD. Jack had interrupted his father’s routine. Thus, Jack expected his father to be devastated, because he would have been.
Bogdashina, O. (2011) 45% …believes that having a new experience gives perception a new and different emphasis. Like the same handful of sand that is formed into different patterns. She says that we learn how to restructure experiences in order to reflect what is needed from us in the environment. New interpretations give us many different perspectives of reality compared to the ‘bubble’ formed around us so we perceive only the reflection of our own world view; such as autistic individuals tend to do.
References:
Baron-Cohen, S. (1995). Mindblindness: An essay on autism and theory of mind. Cambridge, MA; London: The MIT Press.
Bogdashina, O.( 2011). Autism and the Edges of the Known World: Sensitivities, Language & Constructed Reality; eBook.
Cariello, C.(2015). What Color is Monday? How Autism Changed One Family for the Better; eBooks.
Cariello, C. & Capell, J. (2015). Someone I’m With Has Autism; eBook.
Davide-Rivera, J. (2013) Twirling Naked in the Streets & No One Noticed; Growing Up with Autism; eBook.
Staff Writer (2008). Social Issues; Kennedy Krieger Institute. Retrieved online from: https://www.kennedykrieger.org › stories › social_issues
DISCLAIMER (2024) Know Autism – Know Your Child: with < My Thoughts > by Sara Luker; 2024
Just to let you know that I, Sara Hayden Luker, have put forth my best efforts in presenting what I have learned about autism, by sharing the stories and studies of those who have gone before us. Any author’s mention of products, services, treatments, and interventions or actions are not to be considered an endorsement, thereof. Know that to some, autism is an ‘unregulated business’. The content of this website material, digital or in any other form does not represent medical advice; nor does it constitute medical suggestions in any way. The material, including any downloadable parts, is for informational and/or educational purposes only. Your download and/or use of any of this material indicates your acceptance of this disclaimer.
This is a Personal Use Electronic Download. By downloading, you hereby agree and acknowledge that you are not acquiring any right, title or interest in, or to, the material; nor any associated copyrights, other than the right to possess, hold and use for personal, non-commercial purposes. Furthermore, you agree that you will: (i) not scan, copy, duplicate, distribute or otherwise reproduce the material(s) to resell, (ii) not use the material(s) for any commercial purposes. By purchasing/downloading you agree to these terms unconditionally. No ‘rights’ are given or transferred.